
Why do bone metastases hurt?
Most of us have seen patients with severe bone pain from metastatic cancer. And yet few of us have wondered why that pain is present. In this episode, we tackle the question why do bone metastases hurt?
A review of anatomy will help. Around the bone is the periosteum, a very thin layer of cells and fibrous tissue that has a relatively rich nerve and vascular supply. Underneath the periosteum is cortical bone. This area contains thick, densely-packed layers of mineral deposits and is where most of the hardness of bone comes from. The center of the bone is spongy bone, which is made up of looser webbed networks of bone with gaps filled in by bone marrow, which of course produces new blood cells.
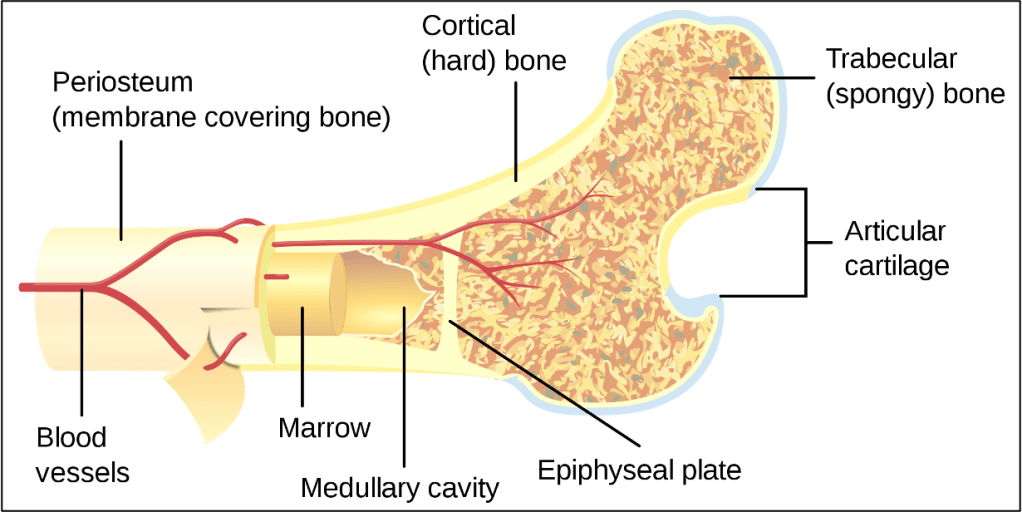
For every 100 nerve fibers in the periosteum, there are only 2 in the spongy central area of the bone and 0.1 in the compact cortical bone. This means that if you were to have a transverse fracture of your humerus, you would break through all 3 of these layers and the majority of your pain would come from the displaced periosteum. This is one of the reasons that early fixation helps not just with healing but also with pain.
But how is that different from bony metastatic pain? Bone pain from a fracture is typically sharp and localizable; someone can tell you exactly where it hurts. Bony metastatic pain can be diffuse, pressure-like, and sometimes hard to localize. For example, in one study that surveyed patients, the top adjectives used for bony metastatic pain were “annoying, gnawing, aching, and nagging.” So we know that the pain syndromes themselves are different.
One key difference is that different kinds of nerves are responsible for the different sensations. There are two big categories of nerve fibers that we see in the bone, A-delta fibers, and C-fibers. A-delta fibers are myelinated, which allows them to carry signals more quickly. Because they can carry signals quickly, they are good for localizing pain. If I hit your arm with a hammer, your A-delta fibers would quickly catch it so that you could move away from the stimulus.
C-fibers are more meandering: they don’t have myelin and are small fibers that can carry pain signals often from a broader area. If I lit a match under your arm, you’d start to slowly feel it over a few seconds because C-fibers pick up heat and chemical stimuli. And because they are not myelinated the signal to your brain is slower.
A-delta fibers are responsible for the initial, sharp pain, and C-fibers are responsible for the slow soreness of recovery. But with metastatic pain, things are more complex.
A series of experiments in the 1970s and 1980s with the marrow of dogs tested the bone marrow pain fiber response to a variety of stimuli different than a typical fracture. Researchers injected saline into the bone marrow of dogs to increase the pressure. They found that by doing so, they were able to detect pain signals returning from the bone. They did the same with chemical stimuli that are known to be noxious elsewhere in the body. Based on this work, it appears that C-fibers and A-delta fibers in the bone, like in other parts of the body, are subject to pressure and chemical stimuli.
So what’s lighting the proverbial match under the bony metastasis? In bone metastases, especially lytic bone metastases, There is a constant balance in the bone between osteoclasts, which break down old bone, and osteoblasts, which build up new bone. Osteoclasts resorb the bone using an acidic environment to break down the mineral deposits. Tumor cells stimulate RANK ligand-RANK binding, which causes osteoclasts to mature. This results in increased bone resorption and a more acidic environment in the bone marrow. That acidic environment stimulates C-fibers and causes bone pain.
Other, less well-understood ways that tumors can cause bony pain are by the direct release of pain-stimulating factors into the local environment. One example is nerve growth factor (NGF) which has been shown to directly stimulate types of C-fibers, and by growing on and compressing nerves directly. These alternate mechanisms may be especially important in osteoblastic metastases, where there is less osteoclast activity and more nerve growth and neorevascularization.
Take Home Points
- Cancer bony pain is a multifaceted entity that takes a variety of different forms and has many physiologic mechanisms. It is different from fracture pain!
- Sharp pain, as one might see with a bone fracture, is transmitted by A-delta fibers, whereas dull, diffuse pain is transmitted by C-fibers.
- These fibers can be activated in different ways by mechanical, pressure, and chemical stimuli.
- Some of the bony metastatic pain is probably the result of local acidosis from bone resorption as well as pressure in cases of “packed marrow.” This explains why it feels different than typical sharp bone pain, and how it can happen even when the periosteum is not involved.
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (0.5 hours), Non-Physician Attendance (0.5 hours), or ABIM MOC Part 2 (0.5 hours).
Listen to the episode
Credits & Citation
◾️Episode by Hannah Abrams
◾️Show notes by Hannah Abrams and Tony Breu
◾️Audio edited by Clair Morgan of nodderly.com
Abrams HR, Breu AC, Cooper AZ. Acetabular Ache. The Curious Clinicians Podcast. September 14, 2022.
Image credit: https://kashpersky.com/bone-cross-section-for-radius-digital-science
