
Why can hypertriglyceridemia cause pancreatitis?
In this episode, The Curious Clinicians dive into a question that occurred to Avi when he was a resident at the VA, sitting in morning report. We break down why elevated serum triglyceride levels, or hypertriglyceridemia, can cause acute pancreatitis.
The first association between pancreatitis and elevated lipids was proposed way back in 1865. But the specific association with triglycerides was only proposed in 1975. The study was published in the journal Surgery. Given how long ago the study was conducted, we don’t have access to the full protocol, and the way the study was designed could raise some ethical questions. This group was actually trying to find out the cause of alcohol-related pancreatitis. Because heavy alcohol consumption is known to increase serum triglycerides, they theorized that triglycerides mediate alcoholic pancreatitis. So they recruited 12 patients who had a history of alcohol pancreatitis, and fed them a diet super high in lipids to see if they got pancreatitis. 11 of the 12 developed triglyceride levels above 600 mg/dL and 7 of them got pancreatitis. So it seemed like the high triglyceride levels had induced pancreatitis.

Zooming forward in time, we now know that hypertriglyceridemia accounts for up to ⅓ of all cases of pancreatitis. And there actually seems to be a dose-response relationship, based on a prospective cohort study from 2012 in the journal Pancreatology. So the higher the level of serum triglycerides, they found the higher the risk of pancreatitis. The classic threshold is an increased risk beginning at around a triglyceride level of 500 mg/dL, and a significantly increased risk above 1000 mg/dL.
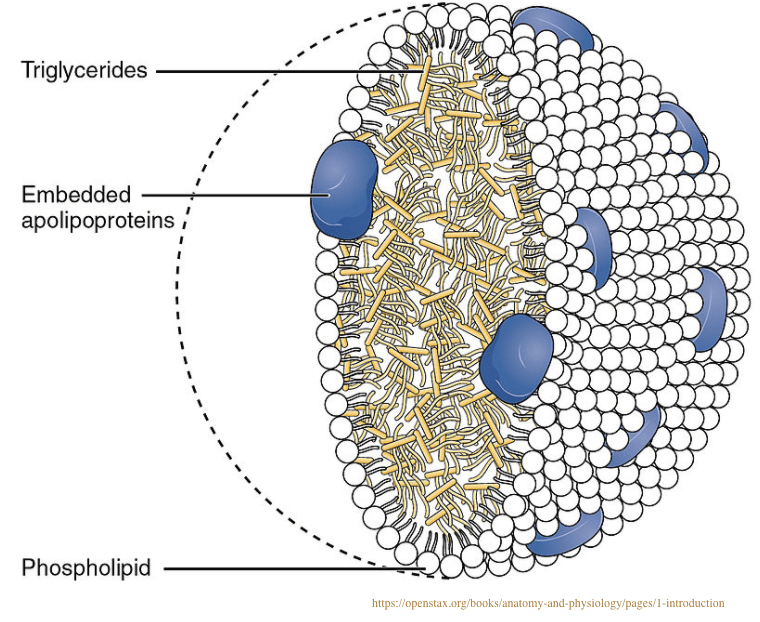
It’s worth reviewing what triglycerides actually are. Triglycerides are a type of lipid and are composed of fatty acids and glycerol. They get absorbed from the food we eat by the small intestine and then are packaged and transported in the blood inside a type of lipoprotein called chylomicrons. These triglycerides inside chylomicrons then get hydrolyzed and broken down to free fatty acids and glycerol by an enzyme called lipoprotein lipase, which can be found on the endothelium near muscles and adipose tissue, where free fatty acids can be stored or used for cellular fuel.

Triglycerides themselves don’t seem to be toxic to the pancreas. But there is evidence that free fatty acids, which get released when triglycerides are hydrolyzed and broken down, are capable of inducing pancreatic injury. This was suggested by three interesting animal studies. The first was from 1991 in the Journal of Surgical Research, where pigs were administered a high concentration of oleic acid, which is a type of free fatty acid, directly into their pancreatic arteries. Some pigs just got control injections. And the researchers found that the pigs who got the free fatty acid injections reliably developed pancreatitis, when compared to the controls. So pretty convincing that free fatty acids can harm the pancreas. The second was a study from 2009 from Acta Physiologica, which was a physiology journal published out of Oxford. They took mouse pancreatic acinar cells, which produce digestive enzymes for the pancreas’s exocrine function, and exposed them to increasing concentrations of oleic acid, that same free fatty acid used in the 1991 pig study. The researchers found that there was dose-dependent damage to the cells, with higher free fatty acid concentrations leading to more damage and more release of amylase and lipase.
The 3rd study sort of confirmed the above findings in a roundabout way. It was published in Science Translational Medicine in 2011, where the researchers took mice and induced pancreatitis with inflammatory cytokines. They then gave the mice the lipase inhibitor Orlistat, which is a drug used to treat obesity. As a lipase inhibitor, orlistat reduces triglyceride hydrolysis and free fatty acid production. And they found that orlistat reduced pancreatic injury, again supporting the role that free fatty acids play in the ability to injure the pancreas.
But we still need to examine why free fatty acids can damage the pancreas. The main proposed mechanisms are trypsin activation and membrane lipid peroxidation.
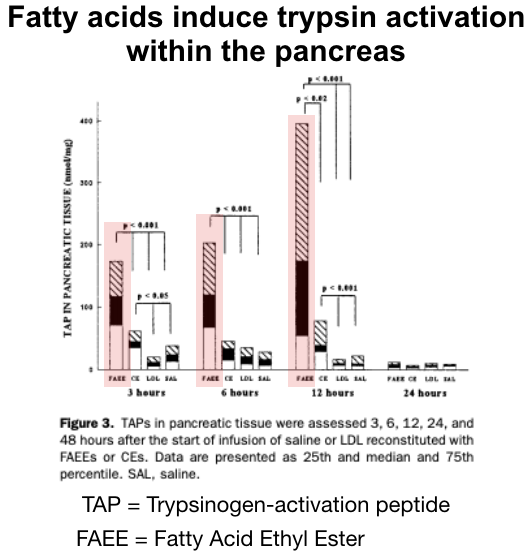
It turns out that free fatty acids actually are able to activate trypsinogen to become trypsin, which was demonstrated in a 1997 study in the journal Gastroenterology. The researchers looked at rat pancreases, and found that infusing fatty acid ethyl esters, which are sort of a form of free fatty acids, into rats led to pancreatitis. And when they looked at the rats pancreases, they found that the fatty acids had activated trypsinogen to trypsin, which then was able to auto-digest the pancreas and set off a cascade that further propagated the initial injury.
Free fatty acids are also able to induce peroxidation of cellular membrane lipids in pancreatic acinar cells. This involves forming free radicals and stealing electrons from membrane lipids in the pancreas. This leads to oxidative degradation of those lipids, membrane damage of the acinar cells, and then necrosis and cell death. All of which is not good for the health of the pancreas.
There actually are additional proposed mechanisms for how hypertriglcyeridemia can cause pancreatitis. Not surprisingly, inflammation is almost certainly involved as well. And an inflammatory response to the initial damage from free fatty acid toxicity in the pancreas probably helps push things over the edge into full blown pancreatitis. Things like cellular damage and death cause the release of cytokines, chemokines, and Damage Associated Molecular Patterns or DAMPs, which leads to neutrophil and macrophage activation, more cell death and damage to the pancreas, and a vicious cycle toward acute pancreatitis.
There are several other theorized explanations as well. These include hyperviscosity from chlymicronemia if the triglyceride level in the blood is really high, which can sludge in pancreatic capillaries and causes obstruction and ischemia. There are also are theories about endoplasmic reticulum stress leading to mitochondrial dysfunction. And there may be genetic predisposition to pancreatitis from elevated triglycerides as well.
When patients come in with pancreatitis from severe hypertriglyceridemia, we often give them insulin infusions in addition to standard supportive care like IV fluids and early enteral nutrition. How does insulin improve this situation?
The most straightforward answer is insulin is really effective at decreasing triglyceride levels in the blood. It does that by increasing the synthesis of lipoprotein lipase, which hydrolyses triglycerides. But, there’s an interesting wrinkle that ties in with the mechanisms we’ve learned about, specifically around how free fatty acids are toxic to the pancreas. It turns out that insulin also inhibits lipolysis from fat, reducing the production of free fatty acids that would have come directly from fat cells. I’m not sure how much of an impact that component of insulin’s mechanism of action has but I thought it was a nice way to link things together.
Take Home Points
- Triglycerides do not themselves cause pancreatitis
- But hypertriglyceridemia does induce pancreatitis via multiple mechanisms.
- These include increased free fatty acids (FFAs), which convert trypsinogen to trypsin, leading to autodigestion and pancreatic inflammation.
- FFAs also induce membrane peroxidation and pancreatic acinar necrosis
- Other contributors include pancreatic capillary hyperviscosity and sludging from hyperchlymicronemia and possible ER stress and mitochondrial dysfunction
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (0.5 hours), Non-Physician Attendance (0.5 hours), or ABIM MOC Part 2 (0.5 hours).
Listen to the episode
Credits & Citation
◾️Episode and show notes by Avi Cooper
◾️Audio edited by Clair Morgan of nodderly.com
Cooper AZ, Abrams HR, Breu AC, Trigging Out, The Curious Clinicians Podcast. August 31, 2022.
Image credit: https://openstax.org/books/anatomy-and-physiology/pages/1-introduction
Related tweetorial: https://x.com/AvrahamCooperMD/status/1396501343729246212?s=20

Hi,
I just noticed you wrote that Insulin would increase synthesis of lipoprotein lipase, when it actually inhibits the synthesis which goes along with reduced free fatty acids.
Besides Thank you very much for your podcasts and the Website. I’m glad to get the ties between dry facts and pathophysiological explanations.
Greetings from a curious clinician in Germany.
Regina
LikeLike