
What conditions affected Abraham Lincoln?
There are certain figures in history whose health has fascinated medical historians and engendered a lot of speculation. Vincent Van Gogh’s affinity for the color yellow was discussed in episode 4. Other examples are Ludwig van Beethoven and the cause of his deafness and the uncertainty surrounding the death of Mozart or King Tut. But few have prompted more speculation than Abraham Lincoln.
Lincoln’s physical appearance was notable even in his own time. At 6’4” he was considerably taller than most people alive in the 19th century. He had other physical features, some of which are shared by blood relatives, that suggest something syndromic. Even William Herndon, a contemporary and later biographer, wrote that his morphology deserved a medical theory to explain it.
The original theory, and perhaps the most often invoked, is that he may have had Marfan syndrome, an autosomal dominant genetic connective tissue disorder. In 1964 a physician named Harold Schwartz published a paper in JAMA arguing that Lincoln had Marfan. The initial idea actually came from an examination of one of Lincoln’s distant relatives, who was a patient of Schwartz’s. The patient was a male descendant of Mordecai Lincoln, Abraham Lincoln’s great-great-grandfather. He had arachnodactyly (very long fingers) which Schwartz felt was likely due to Marfan syndrome. He theorized that Lincoln had it too.
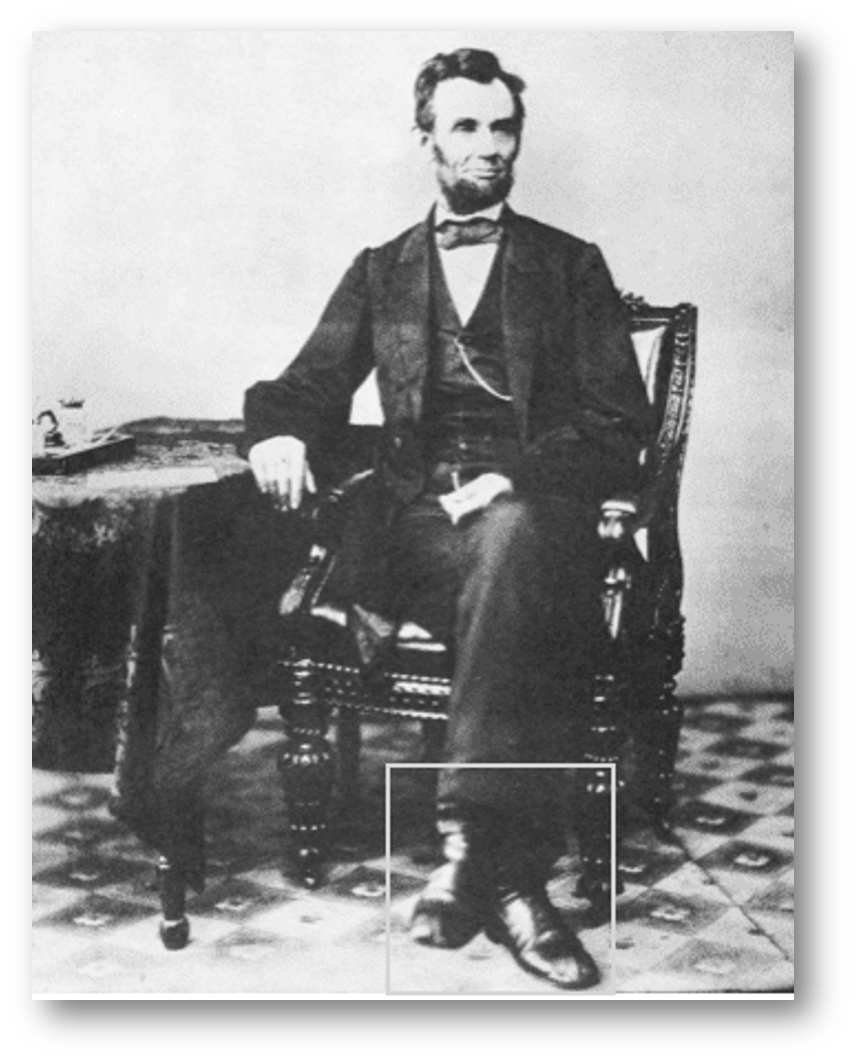
Marfan is now diagnosed using genetic analysis, something unavailable to Schwartz. Instead, he relied on the presence of a marfanoid habitus. The question then becomes: was Lincoln marfanoid? In addition to being very tall and thin, he had very long arms and fingers and a prominent chin. Lincoln also appeared to have flat feet, which can be seen in people with a marfanoid body type. And there is the eponymous Lincoln sign, where someone’s foot bobs with their pulse. This has been loosely associated with aortic insufficiency and/or aortic root aneurysms. The sign is called the Lincoln sign because Lincoln’s foot reportedly bobbed with his pulse. You can see evidence of this where when crossing his knees in photographs his foot looked blurry (see picture below). All of this is consistent with a marfanoid habitus.

There is at least one piece of evidence that argues against Marfan syndrome: Lincoln was far-sighted. Most patients with Marfan’s patients are near-sighted due to effects on the lens of the eye.
The possibility of MEN2b has been raised as well. MEN2b is an autosomal dominant cancer syndrome that presents with marfanoid features and medullary thyroid cancer. The idea that Lincoln may have suffered from MEN2b was proposed in 2007 by a physician named John Sotos, who laid out the theory in a book called The Physical Lincoln. Sotos anchored his theory first in the marfanoid habitus element. He also examined pictures of Lincoln and theorized that bumps around the president’s mouth may have been mucosal neuromas, a common feature of MEN2b. And he referenced the observation that Lincoln’s appearance and general physical wellness appeared to be rapidly declining in 1864 and 1865, in the last year of his life, and theorized that this perhaps represented metastatic cancer, which if present could fit with a cancer syndrome. He later noted in a 2012 article in the journal Clinical Dysmorphology that Lincoln’s mother, Nancy Hanks Lincoln, also appeared to be physically marfanoid in her portraits. Like Lincoln, she was tall and thin and also had very long hands and fingers. She died of a wasting disease at age 34, prompting Sotos to wonder if she had advanced cancer.
It is, of course, a big leap to say that the most likely source of Nancy Hanks Lincoln’s death was a rare cancer such as medullary thyroid cancer. The base rate of infection in the 1800s was much higher. And you can use similar logic for Lincoln’s physical decline at the end of the civil war. He was under a tremendous amount of stress. It seems unnecessary to invoke rare cancers to explain his decline.
Another potential diagnosis is Loeys-Dietz syndrome, a rare genetic syndrome with abnormalities in one of several genes affecting TGF-beta function. It has autosomal dominant inheritance and was actually only described as a unique syndrome in 2005. Patients with Loeys-Dietz syndrome may have vascular, craniofacial, skeletal, or skin abnormalities. And they often have marfanoid features.
There are other clues. Loeys-Dietz syndrome patients are at risk for aortic aneurysms or valvular regurgitation, just like Marfan syndrome patients. And Lincoln had notably widely spaced eyes, a phenomenon known as hypertelorism. Another interesting potential link is craniosynostosis, the premature closure of one or more cranial sutures during infancy. This is a hallmark physical feature in Loeys-Dietz. A paper from 2010 in the Journal of Craniofacial Surgery noted that Lincoln himself very likely had coronal suture craniosynostosis, based on characteristic facial asymmetry with a relative elevation of the superior orbital rim on the involved left side. And the author, Ronald Fishman, examined the pictures of several of Lincoln’s relatives and found 9 individuals across 5 generations with similar asymmetries and likely premature cranial suture closure.
Because of changes in the composition of connective tissue in Loeys-Dietz syndrome, they are known to have very soft and velvety skin. Lincoln’s post-mortem examination was mostly focused on the bullet wounds to his skull and brain, but one of the physicians present, a surgeon named Edward Curtis, noted Lincoln’s skin to be “smooth and clear”. Loeys-Dietz patients often have milia, most commonly on their face. Could the small bumps on and around Lincoln’s mouth and lips represent milia?

One other common craniofacial feature of Loeys-Dietz syndrome is cleft palate. Lincoln’s fourth son Tad had a severe speech impediment. This was well-described by observers at the time and seemed to co-exist with other evidence of what we now think of as developmental delay. John Hutchinson, a speech pathologist, performed a detailed analysis of Tad Lincoln’s reported speech patterns, published in 2009 in the University of Illinois Press. He noted that it’s fairly certain that Tad had a cleft lip. You can see that in his pictures. And of course, cleft lips do often coexist with other mid-line craniofacial abnormalities such as cleft palates. We do not know whether or not Tad had a cleft palate, but Hutchinson made the case that he very likely did, based on the observed patterns of his speech in combination with the existence of a cleft lip. This is another piece of circumstantial supportive evidence toward Loeys-Dietz syndrome in the Lincoln family.
One way to definitively know what condition, if any, Lincoln suffered from is to analyze his DNA. There is a fair amount of Lincoln’s genetic material available. The National Museum of Health and Medicine in Silver Spring, Maryland has a lock of his hair that was removed at Lincoln’s autopsy, as well as bone fragments from Lincoln’s skull that was used by the War Department as evidence of Lincoln’s assasination. They also have the blood-stained sleeve cuffs of Edward Curtis, the surgeon who described Lincoln’s skin at his autopsy. But quite understandably these have not been released for genetic testing. The Secretary of War at the time of Lincoln’s death, Edwin Stanton, famously said after he passed away that “now he belongs to the ages”. This is of course true, but that doesn’t mean we have the right to examine his DNA.
Take Home Points
- The main differential diagnosis for Lincoln’s appearance involves normal variant, Marfan’s syndrome, MEN2b, and perhaps Loeys-Dietz syndrome
- The theory we described on this episode explored Loeys-Dietz syndrome as a novel explanation for his physical features, including marfanoid habitus, craniosynostosis, possible milia around the mouth, and physical features in several family members including a possible cleft palate in his son tad
- But in the end, we don’t (and can’t) really know what, if any, genetic syndrome Abraham Lincoln had
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (0.5 hours), Non-Physician Attendance (0.5 hours), or ABIM MOC Part 2 (0.5 hours).
Listen to the episode
https://directory.libsyn.com/episode/index/id/23964438
Credits & Citation
◾️Episode by Avi Cooper
◾️Show notes by Avi Cooper and by Tony Breu
◾️Audio edited by Clair Morgan of nodderly.com
Cooper AZ, Abrams HR, Breu AC. A Lincoln Theory The Curious Clinicians Podcast. August 3, 2022.
Related tweetorial: https://x.com/AvrahamCooperMD/status/1161836606812299264?s=20

2 thoughts on “Episode 54 – A Lincoln Theory”