

Why does pulmonary embolism cause hypoxemia?
It almost seems unnecessary to ask why an acute pulmonary embolism causes hypoxemia. There’s a clot in the lungs; of course there is going to be an issue with oxygenation. But, as soon as you begin to interrogate the physiology, it becomes quite clear there is a lot more going on. And the explanation has interesting and important implications for treatment.
One of the first clues that there is more than meets the idea is the realization that it is NOT the areas with the acute clot that are causing hypoxemia. It is the unaffected areas. This idea was first proposed by Burton in 1984.
But before we explore this more fully, it would be valuable to review the main mechanisms by which hypoxemia can be caused. There are many approaches to hypoxemia and one of the most commonly encountered is a physiology-based framework. Using this, there are five mechanisms of hypoxemia: decreased FiO2, hypoventilation, V/Q mismatch, decreased diffusion, and shunt.
Many imagine that acute pulmonary embolism (PE) leads to hypoxemia as a result of a shunt. But, acute PE is the opposite of a shunt. To understand this, imagine one were to zoom in to a single respiratory unit with one blood vessel and one alveolus. Now imagine that the blood vessel experienced an embolism and became obstructed by a clot. Notice that ventilation should be normal, but the perfusion distal to this clot should be zero. So, the V/Q is high, maybe even infinity. And remember that shunt is the exact oppositive. Shunts are areas with no ventilation and normal perfusion. The V/Q is zero.
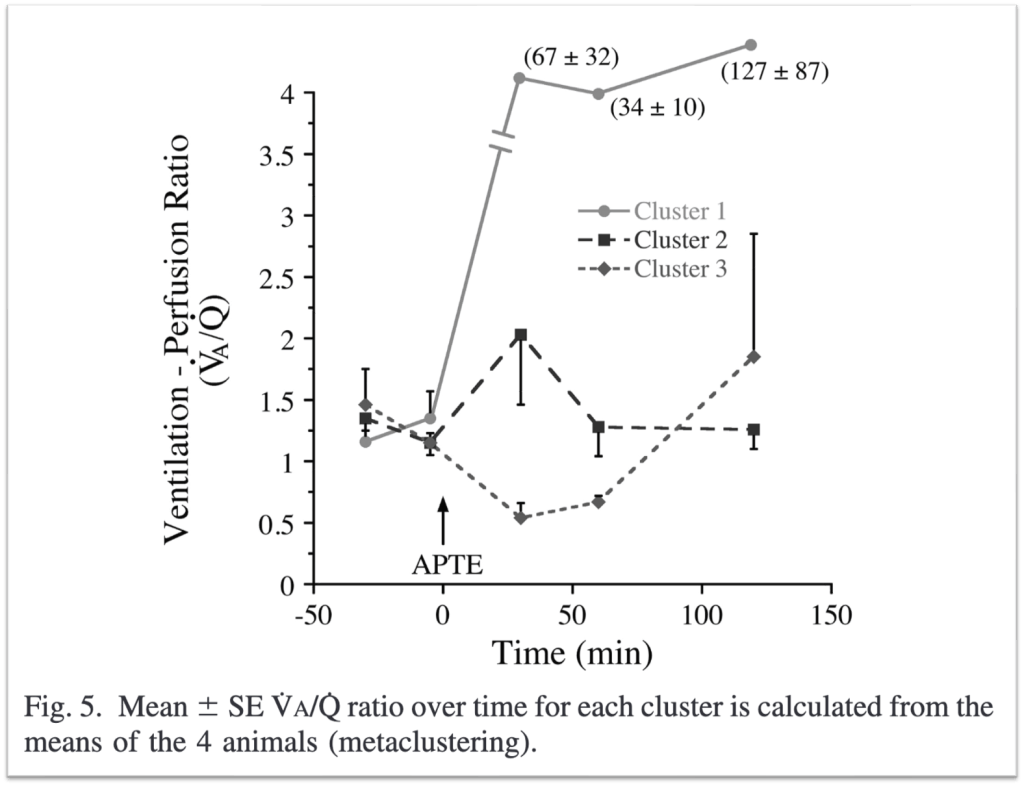
Animal studies involving experimental pulmonary embolism provided much of the data advancing our understand of hypoxemia in acute PE. As can be seen in the Figure 5 from a study by Tsang et al, the V/Q rises dramatically in regions affected by an acute PE.
In some of these studies, the animals are sedated and mechanically ventilated so they cannot alter their minute ventilation. When this is done, one of the first things seen is an increase in pCO2, or hypercapnia. The increased pCO2 is found in the areas with the clot; this is to be expected once we know that these will be areas of normal to increased ventilation but low to no perfusion.
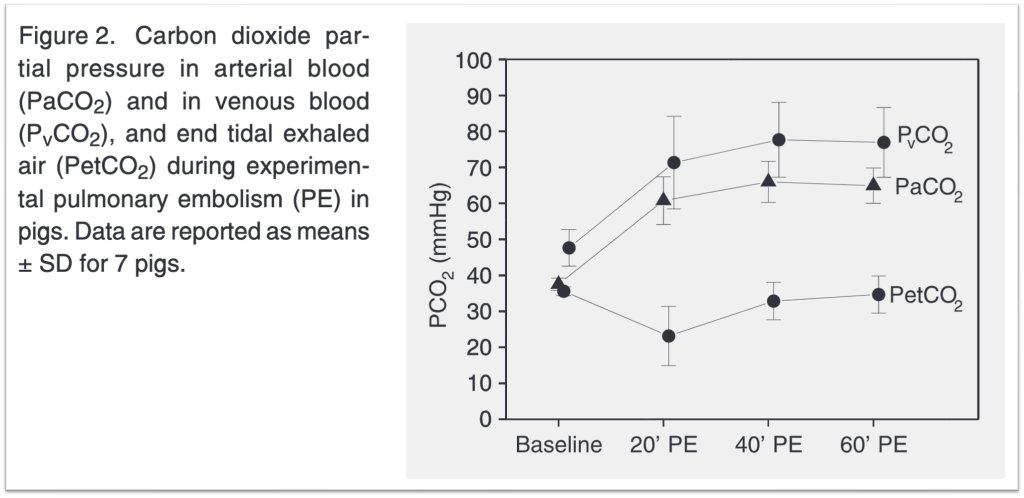
Supporting this are also case reports of patients who experience PE while on a vent. A marked rise in pCO2 can be seen. The resulting hypercapnia may be one reason reason people with acute PE often present with tachypnea.
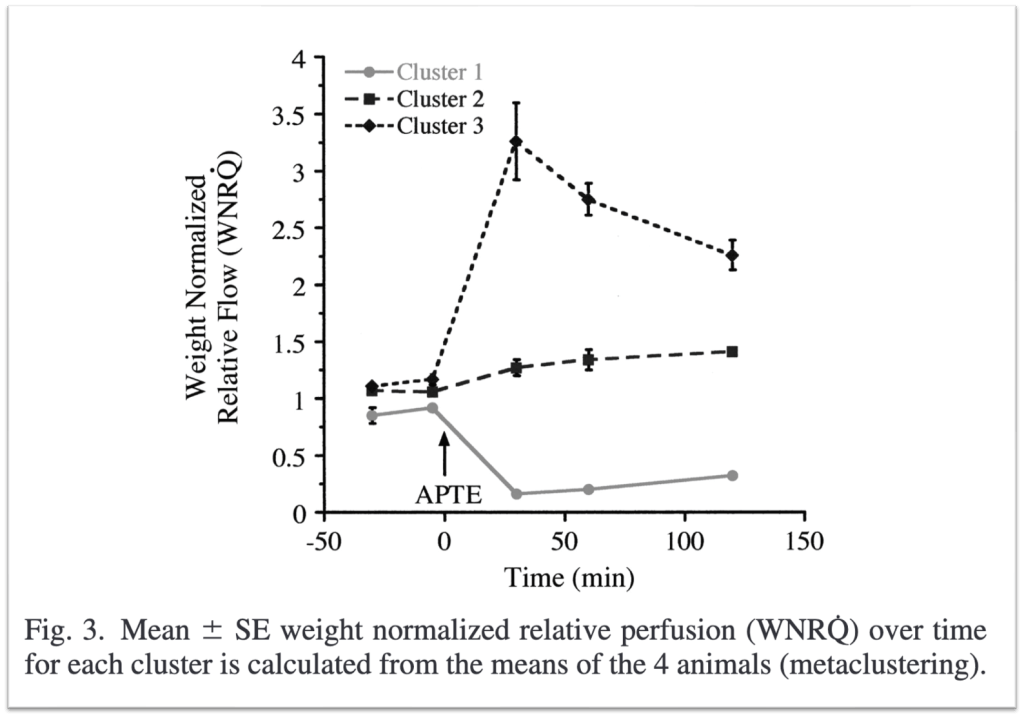
Zooming back into the unit with the clot, given given that the blood cannot traverse the obstructed blood vessel it is diverted to other regions of the lung.
Going back to the animal studies mentioned earlier, the investigators found that in addition to areas with clots having low flow or Q the the areas without clot experienced an increase in flow. In essence, the blood that is blocked by the clot goes to areas of the lung that do not have a clot.
And because the ventilation (V) in these zones should be unchanged, at least initially, and the pefusion (Q) is increased, overeall there is a decreased V/Q ratio. And units with low V/Q are those that classically lead to hypoxemia. This is exactly what’s seen in the animal studies. The areas without clots have low V/Q ratios and are the areas of hypoxemia.

Now imagine a scenario where a patient with massive acute PE has shock. They’re placed on a positive inotrope, like dobutamine. What will happen to their SaO2?
It could go down.
If you increase perfusion (Q) by giving an agent that increases cardiac output, you might see a worsening of the V/Q mismatch discussed above. This has been demonstrated in animal studies and in case series.
This explanation might also explain something many of us have observed: patients with acute PE, even massive PE, may not have hypoxemia. If hypoxemia only results from the diversion of blood away from areas of thrombus, one might imagine a scenario where this has not occurred. If so, no hypoxemia would be seen. Also, that blood might not be contributing to cardiac output. This sort of patient is exactly the type that would present with obstructive shock.
Take Home Points
- In acute pulmonary embolism, blood is diverted away from the area with clot.
- This creates an increase in perfusion (Q) without a matching increase in ventilation (V).
- The result is a decreased V/Q ratio and hypoxemia.
- Notably, the areas of low V/Q are those unaffected by clot.
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (0.5 hours), Non-Physician Attendance (0.5 hours), or ABIM MOC Part 2 (0.5 hours).
Listen to the episode
https://directory.libsyn.com/episode/index/id/23801888
Credits & Citation
◾️Episode and show notes by Tony Breu
◾️Audio edited by Clair Morgan of nodderly.com
Breu AC, Abrams HR, Cooper AZ. Very/Qurious Hypoxemia The Curious Clinicians Podcast. July 20, 2022.

One thought on “Episode 53 – Very/Qurious Hypoxemia”