
How does Wenckebach happen?
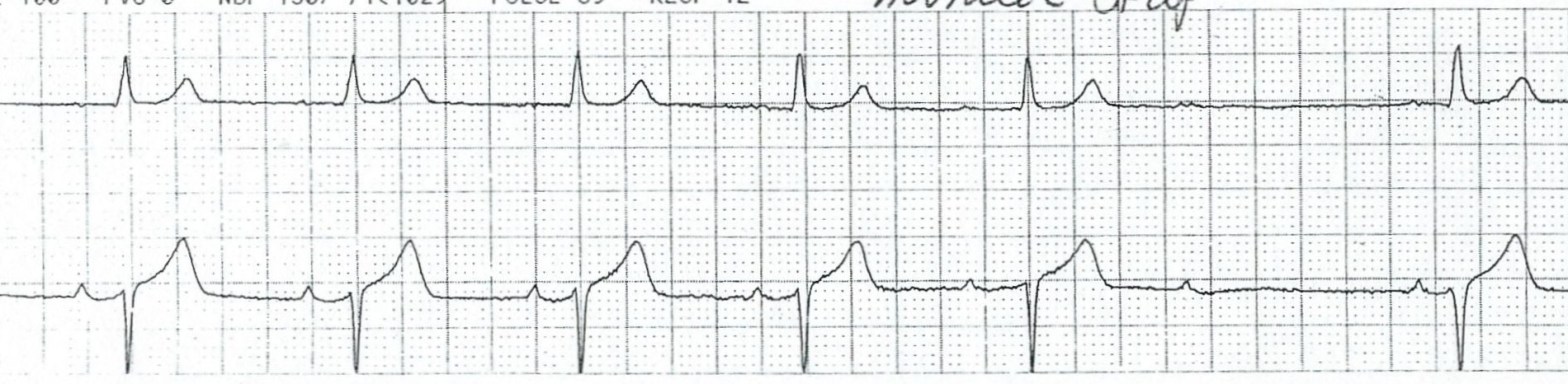
Wenckebach is a fascinating cardiac rhythm. It is a form of heart block with progressive, beat-to-beat prolongation of the PR interval. Eventually, after this progressive PR prolongation, one of the P waves fails to conduct. After this non-conducted P wave, the cycle repeats with a return to the original PR interval length followed by prolongation again. The question becomes: how does this happen?
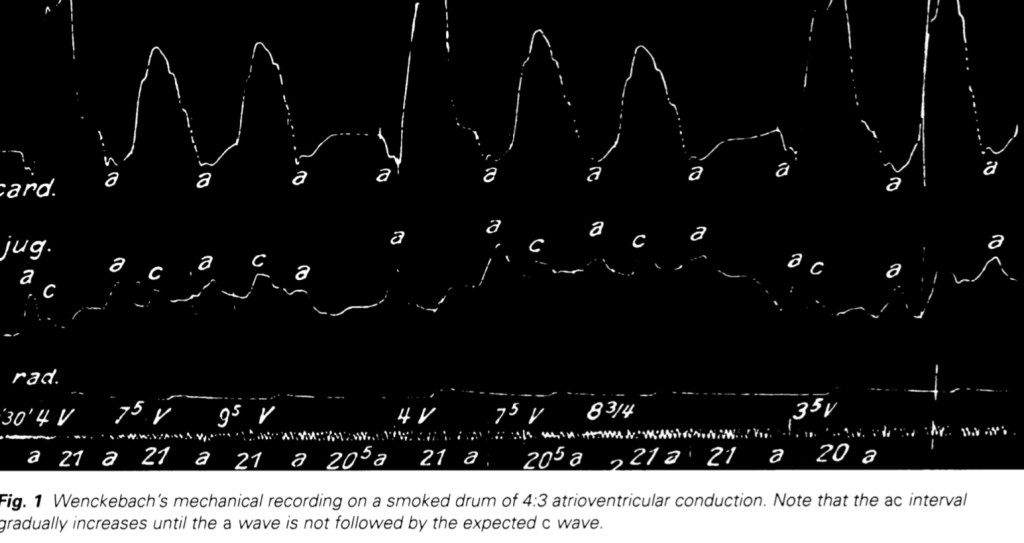
Before attending to the mechanism behind Wenckebach, a brief review of its history and initial description is in order. Karl Frederik Wenckebach was a Dutch anatomist and physician who, in the late 1800s, was on faculty at the University of Groningen in the Netherlands. We know about him because of fundamental clinical observations about the heart though his first love was pathology. Because he was colorblind he had a hard time discerning different types of tissue under the microscope and so gravitated toward the black and white tracings of cardiovascular physiology. And in 1898 he was caring for a patient and noticed something peculiar when examining their pulse: he found it to be irregular but with a type of repeating pattern that he had not encountered before. It was regularly irregular and had a repeating pattern with a progressive delay between the a-wave of the jugular vein pulse and carotid pulsation. This delay became longer and longer with each beat until there was an a-wave without carotid pulsation. And this cycle repeated itself with a 4:3 pattern such that every 4th beat was dropped. He traced this out mechanically on a smoked drum or a kymograph and published the description in 1899, and it corresponds exactly with what we now know as the Wenckebach pattern.
Wenckebach is also known as Mobitz type I. Woldemar Mobitz was a Russian physician a generation younger than Wenckebach. He had access to early electrocardiograms and in the 1920s described different types of heart block, including one that corresponded to what Wenckebach had described 30 or so years before.
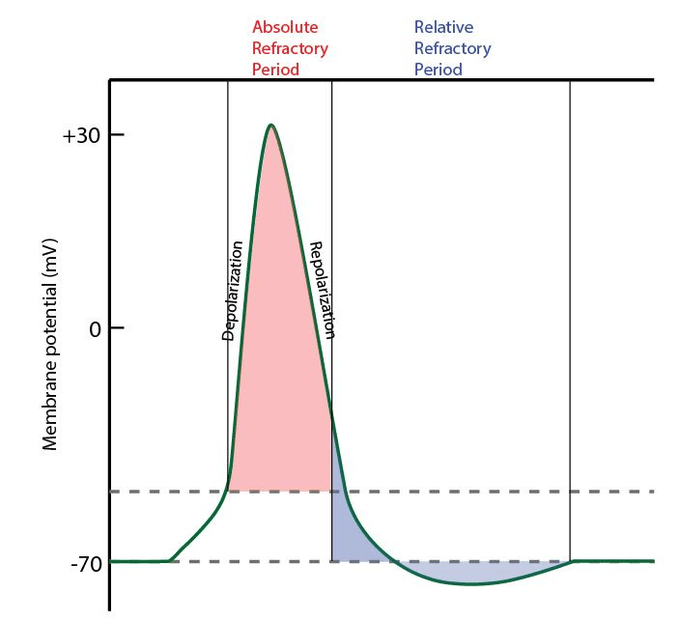
To understand why the Wenckebach rhythm has a unique pattern, one must understand the concepts of absolute refractory period and relative refractory period. The absolute refractory period encompasses most of the action potential within a myocyte. In technical terms, that would be phases 0, 1, 2, 3, and part of 4. This encompasses almost all of the ventricular cardiac cycle on the EKG, including the QRS and the T wave. Because there are 4 phases of the cardiac cycle, a myocyte spends almost the whole electrical cycle in the absolute refractory period. This represents the period when the cell cannot depolarize at all because sodium influx channels are unable to open.
The relative refractory period, on the other hand, follows the absolute refractory period. Under normal circumstances, depolarization doesn’t happen during the relative refractory period either but rather occurs right after it ends, before a new absolute refractory period begins again. Depolarization can happen during the relative refractory period, but those sodium channels are still relatively closed and harder to open. So a depolarization during the relative refractory period leads to a weaker, slower electrical impulse than normally timed depolarizations.
The AV node is crucial for the formation of Wenchkebach. Normally, to allow for efficient and coordinated pumping of blood in the heart, electrical impulse conduction via action potentials through the AV node is rapid (approximately 0.05 m/sec), though this is slower than in other parts of the heart. This allows the atria to fully empty before the ventricles contract.
If one were to imagine what would happen if conduction through the AV node slowed as a result of an issue affecting the AV node (e.g., intrinsic conduction disease, vagal tone, ischemia, or medications like beta-blockers). In this situation, depolarization should still occur in the AV node but would be delayed and weaker.
An electrical stimulus arriving to a slowed AV node will extend the duration of the action potential. When the next electrical stimulus arrives, it still occurs and transmits through the AV node but instead of occurring AFTER the relative refractory period of the first action potential, which is the normal order of events, the second depolarization occurs DURING the relative refractory period.
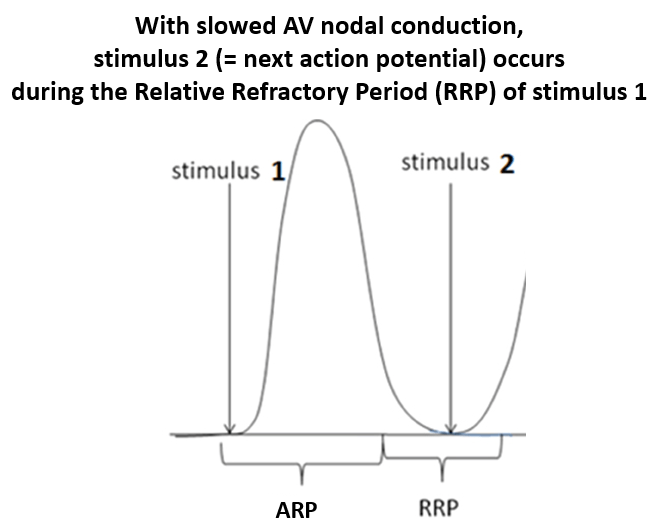
This leads to the first manifestation of the Wenckebach pattern. If you have depolarization within the AV node during the relative refractory period, this decreases the strength and amplitude of the depolarization and increases its duration. This manifests in delayed conduction of the atrial impulse to the ventricles and a longer action potential. Both of these prolong the PR interval. The PR interval of stimulus 2 is longer than it was for stimulus 1. When a third action potential arrives at the AV node, the same issue occurs.
Depolarization again occurs within the relative refractory period of the previous action potential, which further weakens and delays conduction of the atrial impulse and extends the PR interval even more. And because the depolarization is delayed and the relative refractory period keeps getting longer, each subsequent depolarization occurs earlier in the relative refractory period.

With each subsequent depolarization, the action potential has been weaker and slower and happening earlier and earlier in the relative refractory period. At some point, often by the fourth beat in the cycle, the depolarization signal arrives at the AV node in the absolute refractory period. Nothing will happen in the absolute refractory period because the sodium channels simply cannot open. This leads to non-conduction of the atrial impulse to the ventricles, which shows up as a “dropped beat” on the EKG. We also can call this a non-conducted p-wave.
And this cycle repeats.

We think about Wenckebach cycle length in terms of the P to QRS ratio, with one fewer QRS than P waves in any given cycle because of that non-conducted P wave at the end of the cycle. Typical ratios are 4:3 or 5:4. Exactly what that ratio will be is determined by when depolarizations shift back into the absolute refractory period. Earlier shifts lead to shorter cycles and a lower ratio (e.g., 4:3). Later shifts lead to longer cycles and a higher ratio (e.g., 5:4).
Take Home Points
- The Wenckebach pattern arises when decreased AV node conduction leads to longer, slower action potentials and depolarization that occurs during the relative refractory period
- This progressively increases the PR intervals with each beat
- Eventually, depolarization occurs during the absolute refractory period and this results in a non-conducted p-wave
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (0.5 hours), Non-Physician Attendance (0.5 hours), or ABIM MOC Part 2 (0.5 hours).
Listen to the episode
https://oembed.libsyn.com/embed?item_id=23642882
Credits & Citation
◾️Episode by Avi Cooper
◾️Show notes by Avi Cooper and Tony Breu
◾️Audio edited by Clair Morgan of nodderly.com
Cooper AZ, Abrams HR, Breu AC. Way Back Wenckebach. The Curious Clinicians Podcast. July 6, 2022.
Image credit: https://ecgguru.com/ecg/wenckebach
