

In this episode, we discussed fevers and chills. More specifically, we asked “why do we feel cold when we have a fever?” Shouldn’t we feel hot? We also discussed the dictum “culture if spikes”, meaning if your patient spikes a fever, blood cultures should be ordered. It is certainly one of the most common contingencies given during signout.
To start, some definitions would be helpful. Chills have been defined as the perception of cold and involuntary muscle tremor. We’ve all experienced this. Typically chills occur when we’re exposed to a cold environment. If you’re in a cold room without a sweater or coat, you might feel cold and start to shiver. If my hypothalamus has my internal thermostat set at 98°F and my core temperature drops because my environment is cold, I’ll feel cold and I’ll have chills. These same experiences can occur as a prelude to fever.
Shaking chills, which are also known as rigors, are a more severe form. It’s one of those things which fall into the category of “you know it when you see it” or “you know it when you experience it”. For those interested in a more formal definition, one study defined shaking chills as “involuntary shivering such that holding a glass of water in the hand would cause the water to spill out.”
Let’s get the order straight
If we obtain blood cultures in response to fever, knowing when the fever occurs in relation to bacteremia would be helpful. More specifically, we must understand the order of events after an episode of bacteremia. For example, when do we feel cold? And, how soon after does bacteremia and chills does fever occur?
To understand the answers, a few points must be reviewed:
- Bacteremia exposes us to exogenous pyrogens. For example, the cell wall of gram-negative rods contains lipopolysaccharide (LPS; endotoxin).
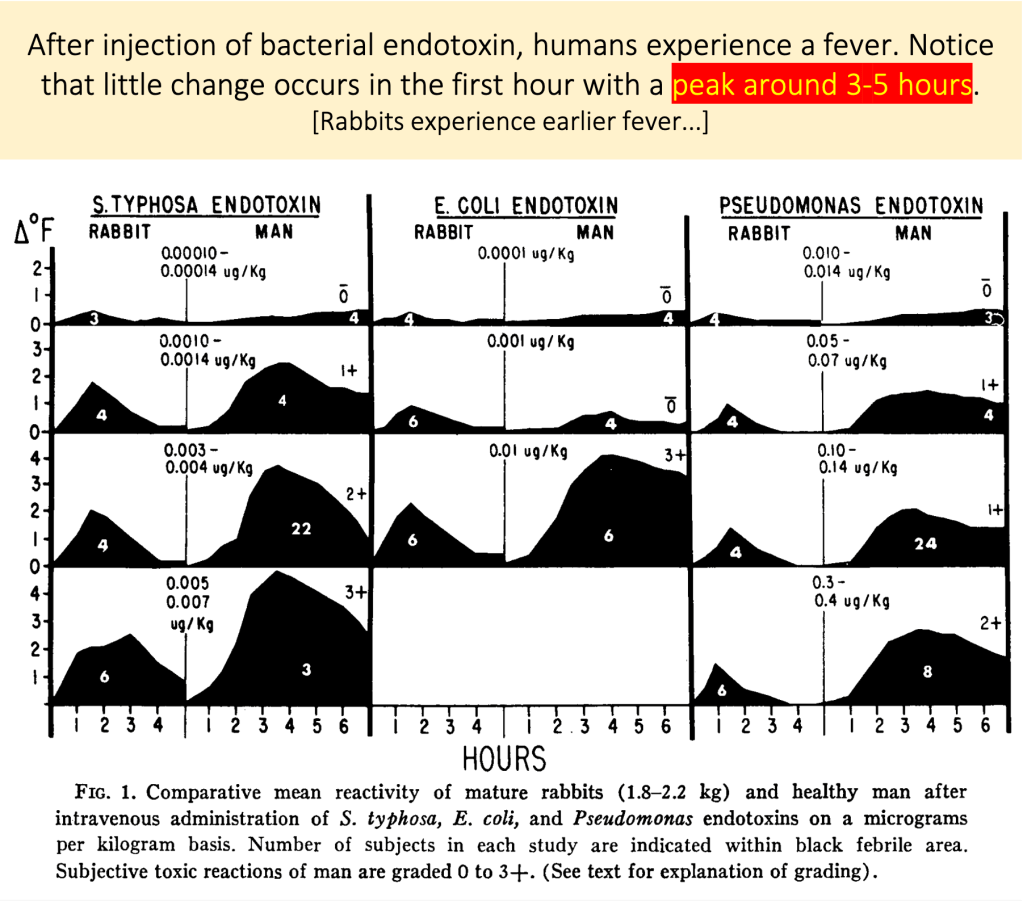
- There is experimental data showing that when LPS is injected into humans, it induces fever. But, very importantly, there is a 3-5 hour delay between exposure and peak fever. It takes time to generate a fever.
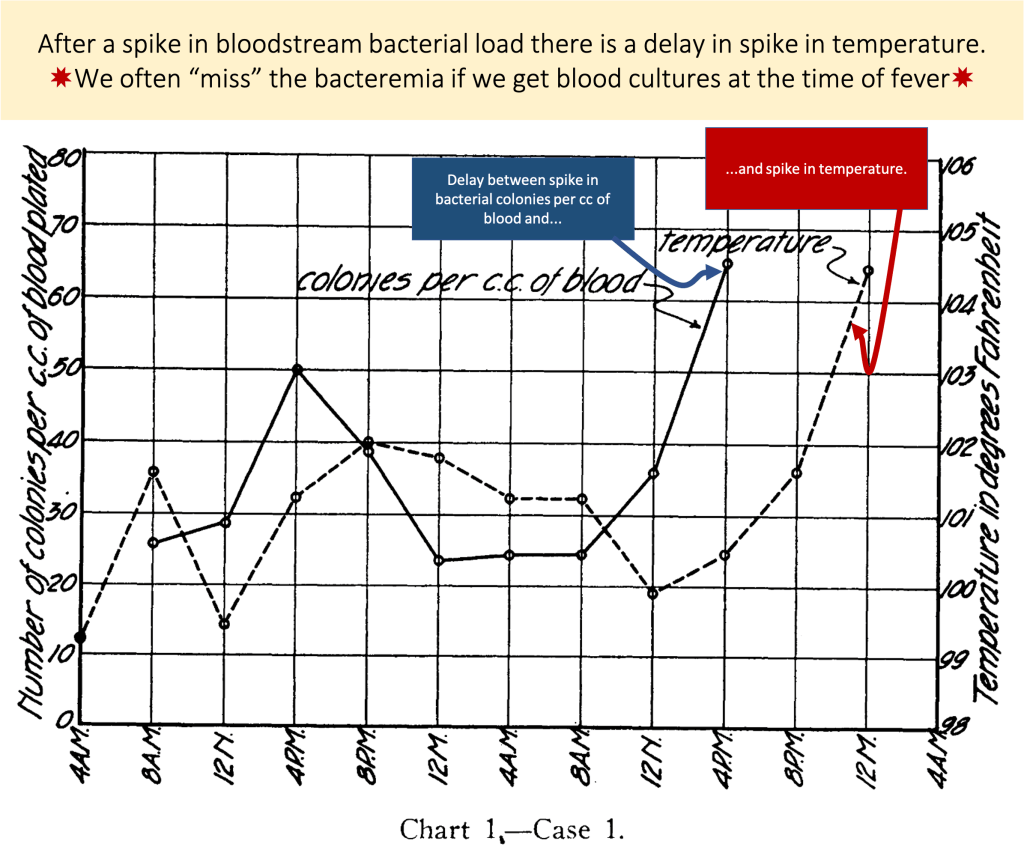
The delay between clinical bacteremia and fever was demonstrated by Harry Weiss and Reubek Ottenberg who studied the association between bacteremia and fever in patients with endocarditis. Their results were published in 1932. They found that there was a delay of many hours between peak bacteremia and fever. They conclude by writing, “The results indicate that if diagnostic blood cultures… are made just before the expected rise in temperature, more positive results and higher bacterial counts will be obtained.”
So… we just need to predict future fever?
While it may seem unlikely that we can predict future fevers (allowing us to obtain blood cultures at a more optimal time), a fuller understanding of the sequence from bacteremia to fever may make it possible.
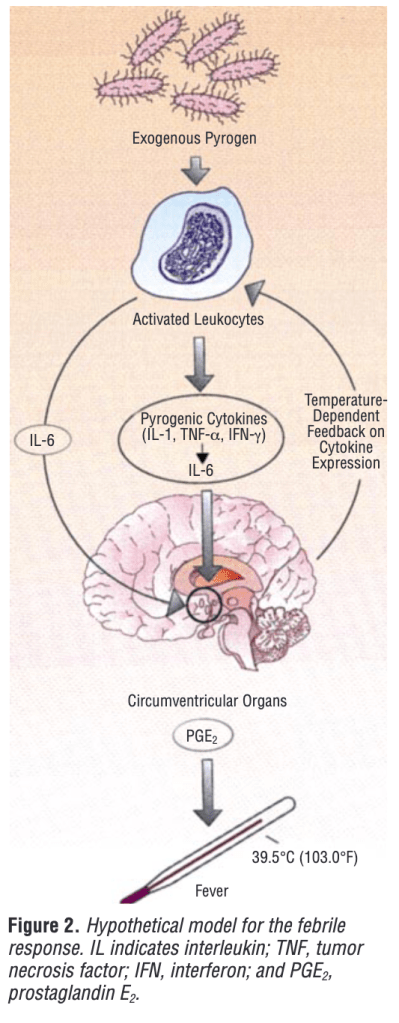
First, bacteria enter the bloodstream exposing us to exogenous pyrogens. LPS is the classic exogenous pyrogen, but other bacterial toxins or viral hemagglutinin are also exogenous pyrogens. These exogenous pyrogens induce endogenous pyrogens. Endogenous pyrogens include cytokines IL-1, IL-6, and others.
These endogenous pyrogens lead to an increase in prostaglandin E2 which acts on the hypothalamus to increase the hypothalamic set-point. So, if the normal hypothalamic set-point is around 98°F, it might be increased to 101°. Because the temperature in the body isn’t actually 101°, it must now do things to get it there.
Because your body is actually cold compared to what it wants to be (e.g., the core temperature is 98°F but the hypothalamus has set the goal at 101°F) this is a form of relative hypothermia.
There is some data suggesting that the signal that makes us feel cold is acting centrally. We feel cold because we are cold, relative to what our set-point is. There’s really no difference between a set-point of 98°F and a core-temperature of 95°F (as you might experience being outdoors in freezing weather for many hours) and a set-point of 101°F and a core temperature of 98°F. Both of these are 3 degrees below where the body wants to be. It makes sense that we’d feel cold.
It’s worth noting that the sensation of cold probably has a teleological explanation: when we feel cold, we seek shelter or a warm blanket. These behavior changes will help to retain heat, helping our body get the set-point where it needs to be.
This also explains shivering. In some situations it won’t be enough to cover ourselves with a blanket. The body needs to do other things. Our bodies vasoconstrict peripherally so that we are less apt to lose heat through our skin. We also generate heat, aka thermogenesis, by shivering
Eventually, these factors raise our temperature. The result is a fever.
Why don’t we all get rigors?
More vigorous chills seen with rigors promote greater thermogenesis. You might really want that with high-grade gram-negative rod bacteremia but need it less for a urinary tract infection.
This is supported by some data. One research study looked at whether fever is predictive of positive blood cultures. Somewhat surprisingly, fever was not predictive. Other studies have found that rigors are more predictive. In situations where a rapid rise is temperature is required (e.g., with high grade bacteremia), rigors are more likely. Based on these differences in predictive value, it might make more sense to “culture if shakes” rather than “culture if spikes”.
Regardless, what should be clear is that the closer to the rigors one gets the blood cultures the greater the probability of a true positive. Fortunately for us, the body is really good at clearing bacteria from the blood. As for fever, once that occurs we’re typically hours from bacteremia. The macrophages of the RES have often done their job by then. It may just be too late to see it with the blood cultures drawn in response.
Take Home Points
- The order of events: bacteremia and exogenous pyrogen exposure → endogenous pyrogen → PGE2 increasing the hypothalamic temperature set-point → chills/rigors → fever
- We may feel cold chills as a cue to drive behavioral change (e.g., put on a sweater)
- Rigors promote rapid heat production
- By the time fever occurs, bacteremia may have already cleared
- Because rigors occur before fever (i.e., temporally closer to bacteremia), they are better predictors of positive blood cultures
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (1.00 hours), Non-Physician Attendance (1.00 hours), or ABIM MOC Part 2 (1.00 hours).
Listen to the episode
Credits & Citation
◾️Episode and show notes written by Tony Breu
◾️Audio edited by Clair Morgan of nodderly.com
Breu AC, Abrams HR, Cooper AZ. Why do we feel cold when we have a fever? The Curious Clinicians Podcast. March 17, 2021.
Image credit: https://www.news4jax.com/news/local/2020/04/04/thermometers-flying-off-store-shelves-during-pandemic/
Related tweetorial: https://x.com/tony_breu/status/1305589726003556354

One thought on “Episode 21: Why do we feel cold when we have a fever?”