
Why does meperidine treat rigors?
When a patient is having rigors that are causing them to desaturate or become tachypneic, you may have turned to meperidine to stop them. Meperidine is an opioid that has fallen out of common use for most indications, but remains a go-to agent for many to stop disadvantageous rigors. How did this drug work for rigors, and why don’t we use other opioids for this indication?
Meperidine was the first synthetic opioid, and it was originally developed in 1939 by chemists in Germany. It rose to prominence in the 1940s as an alternative pain medication and anesthetic to morphine, as a paper from 1943 described: “the increased need for morphine in time of war and the present threat to our opium supply make it important that appropriate consideration be given to the new analgesic [meperidine], for this compound can be prepared synthetically from available chemicals.” From early on, meperidine was noted to have some key differences from morphine: it had an additional antispasmodic effect, was quicker “on/off”, and was initially thought to be less likely to cause dependence, though later that was disproven.
Over time, other opioid analgesics emerged as better options for treating pain, but meperidine remained as a treatment for rigors. Numerous studies have shown its effect for this indication: A meta-analysis of 94 studies and sub-studies of anti-shivering medication randomized controlled trials, covering 30 drugs and drug combinations, showed that across 16 RCTs, meperidine had a risk ratio of 2.2 for likelihood to prevent or treat shivering. To compare to other opioids, fentanyl had a risk ratio of 1.2 (where 1 would be insignificant).
So why might it work better than other opioids? The first step to understanding this is understanding the different opioid receptors and how they work. There are 4 main opioid receptors: Mu, Delta, Kappa, and opioid receptor like-1 (ORL-1). They each share some intracellular signaling pathways after receptor activation, and some which are unique. Mu opioid receptors are the receptor we most commonly talk about when we talk about opioid agonism: activation of MOR is key for alleviating pain, can increase mood, and modulate euphoria. It’s the best studied and understood of the receptors. By contrast, the Kappa opioid receptor (KOR) has a variety of potential implications that are as yet to be determined, including antispasmodic. This matches clinical uses, where KOR agonists are being developed for IBS, and meperidine used to be used for pancreatitis in people who had had sphincter of Oddi spasm with morphine. Interestingly, while MOR agonists notably cause itching, KOR suppresses itching. Meperidine is originally thought of as a mu receptor opioid, but it also has moderate affinity for K and delta opioid receptors, whereas fentanyl and morphine act more purely on Mu receptors.
2 hypotheses can connect this Kappa-Mu difference between meperidine and other opioids to its effect on shivering. One is that the effect on the kappa opioid receptors causes decreased muscle spasms, just like they noticed for urologic surgeries and childbirth during the initial uses of this drug in the 1940s. So with diminished muscle responsiveness, almost a muscle relaxant effect, the muscle would be less ‘excitable’ by a stimulus from the brain that says “you’re cold, time to shiver”. This is supported by experiments that have shown that meperidine decreases the “shiver” threshold in humans.
The other hypothesis is that meperidine interferes with temperature sensing itself. Temperature sensation is transmitted up the dorsal horn nuclei of the spinal cord to the thalamus, which then relays it to the cortex (prompting “seek warmth” behavior) and the hypothalamus (prompting vasoconstriction, adipose thermogenesis, and shivering). As we explained in episode 21, when we have an infection the hypothalamus increases the “set point” for temperature, so our goal temperature is increased and we shiver at a lower temperature. So, while this hypothesis is less studied, it is possible that meperidine and its effect on the KOR is interfering with the very sensation of ‘cold’ itself that drives rigors.
Two key experiments can support the idea that KOR, rather than another opioid receptor, is the reason for the difference between meperidine and other opioids. The first is an experiment in humans, which answered the question: “If we block KOR, can we block the effect of meperidine on shivering?” It used the fact that at low doses, naloxone blocks just Mu receptors, and at high doses, it blocks both Mu and Kappa receptors. They gave volunteers an infusion of cold saline to make them shiver, and then either low- or high- dose naloxone. The people who had gotten high-dose naloxone, so the people for whom KOR activity was blocked, had a minimal improvement in their shivering with meperidine, whereas those who had gotten the lower dose naloxone, in whom just Mu was blocked, saw the full effect.
The second study is a study in rats, which attempted to answer the opposite question: “Does a high dose antagonist of Kappa or Mu opioid receptors cause hyperthermia?” The researchers gave rats a mu-antagonist, CTAP, and a Kappa-antagonist, nor-BNI. They found that rats who got the Kappa antagonist became hyperthermic and mice who got the Mu antagonists became hypothermic. Rats who got both stayed around the same temperature. This also suggests that KOR has some effect on cooling, and that the Kappa and Mu receptors may balance each other. This comes back to meperidine, which has a different K and Mu receptor balance than other opioids. Other Kappa agonists, such as butorphanol (which is not used in humans) also have been shown to work better for shivering than Mu-predominant opioids.
How do we know that temperature sensing leading to shivers are separate from other mechanisms for mounting a fever or staying warm, like vasoconstriction? One study in 1997 wanted to look at this specific question: they gave healthy volunteers meperidine and placebo and then put them into hot and cold rooms. They measured a variety of vital signs including oxygen consumption from shivering. They found that at a higher dose of meperidine, the shivering threshold was much decreased– going down from starting to shiver around 35.5 degrees Celsius in the control group to down to 32 degrees Celsius to shiver at the highest meperidine doses. Interestingly, the effect on vasoconstriction was much less! So patients in that higher group still had vasoconstriction at 35 degrees and the amount of lowering with meperidine was much less. This is different from most other opioids and many other anesthetics, which have a more comparable effect on the threshold to both vasoconstrict and shiver.
Ondansetron and other anti-serotonergic medications came into use for shivering after most trials of meperidine were done, and so less data is available to support their use. However, a more recent meta-analysis has shown that 5-HT3 antagonists can prevent post-operative shivering.
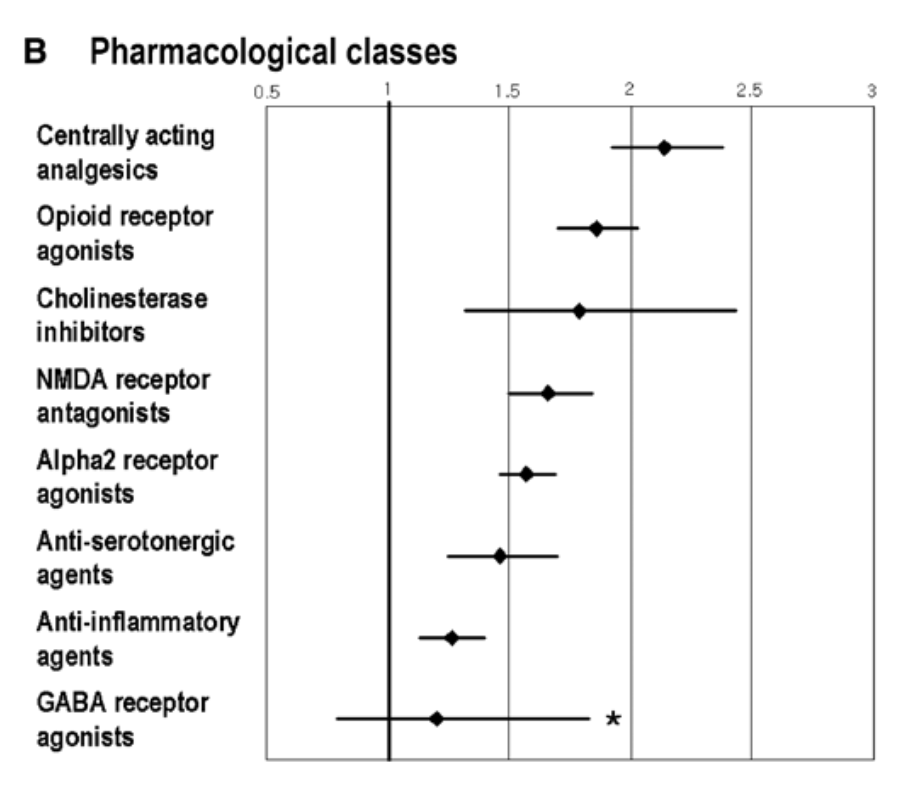
Pharmacological classes’ action on shivering reduction. Park et al. 2012.
Lastly, no discussion of the history of meperidine would be complete without discussing the tragic story of Libby Zion. Libby Zion was a freshman in college who was admitted to the hospital with what was described as a “flu-like illness”. She was admitted by two resident physicians who were taking care of dozens of other patients on a 36-hour call shift. She was treated with meperidine, which interacted fatally with a MAOI she was taking as an outpatient medication, and ultimately died of a serotonin-syndrome like interaction between the two medications. This case was pivotal in hospital safety interventions in the United States and duty hour reform for resident physicians.
Take Home Points
- Meperidine is a mixed mu/kappa opioid which has a disproportionate effect on stopping the shivers
- This effect be result from decreased muscle reactivity mediated by signaling via kappa receptors or interference in temperature sensing
- In certain clinical scenarios this effect of meperidine can be beneficial
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (0.5 hours), Non-Physician Attendance (0.5 hours), or ABIM MOC Part 2 (0.5 hours).
Listen to the episode
https://directory.libsyn.com/episode/index/id/25874010
Credits & Citation
Episode and show notes written by Hannah Abrams
Audio edited by Clair Morgan of nodderly.com
Episode citation: Abrams HR, Cooper AZ, Breu AC. Stopping the Shakes. The Curious Clinicians Podcast. February 8, 2023.
This episode is sponsored by BetterHelp! You can give online therapy a try at betterhelp.com/CLINICIANS.
Cover image source: https://www.gnhindia.com/products/us-ndc/meperidine-hydrochloride-demerol-30698-335/

Having trouble registering &or entering my ABIM no. for getting the CME & MOC point credit needed
LikeLike