
Why can a ketogenic diet help control seizures in epilepsy?
Many forms of dietary therapy make intuitive sense. 18th-century sailors with scurvy were treated with lime juice and other sources of the missing vitamin C. Patients with diabetes mellitus are counseled to avoid foods with a high glycemic index. And those with chylothoraces, where a chylous (fatty fluid) leak into the pleural space causes an effusion, are told to consume low-fat diets to reduce chyle flow and help prevent fluid from re-accummulating.
But why do ketogenic diets help control seizures in refractory epilepsy? This benefit is one of the oldest medical interventions still in use. As far back as 500 BC, the Hippocratic collections mention dietary modifications as a treatment for seizures and even discuss the benefits of fasting. Using ketones to treat epilepsy is truly an ancient intervention. And the result is almost magical, not only in effect but also in the obscure way in which it works.
Ketogenic diets are high in fats and very low in carbohydrates. To be clear, we are discussing therapeutic ketogenic diets rather than low-carb diets meant for weight loss. Ingesting a high-fat, low carbohydrate diet leads to increased serum free-fatty acids. These free-fatty acids get metabolized in the liver to acetyl-CoA and then to acetoacetyl-CoA. Acetoacetyl-CoA then gets converted to 3 types of ketones or ketones bodies: acetoacetate, acetone, and beta-hydroxybutyrate. These ketones can be used as cellular mitochondrial fuel via the Krebs cycle, most notably in the brain. This is particularly important if you’re taking in a diet that is ultra-low in carbohydrates.

A ketogenic diet induces a state of pseudo-starvation. Because the body is primed to use glucose as the primary metabolic fuel, the accumulation of ketone bodies tricks it into thinking food is scarce. Until the 1920s, when insulin was discovered, ketosis was thought to be harmful, since diabetic ketoacidosis was such a dangerous state. And many clinicians are primed to see ketosis as a pathologic state. However, this is not always the case, as intentional ketogenic states demonstrate.
The first inkling that ketogenic diets may help ameliorate seizure burden in epilepsy came from observations of starvation. In the early 1920s, a physician from Michigan named Hugh Conklin incorrectly theorized that epilepsy originated in the intestines, and he thought he might be able to cure it by starving patients. He starved children with epilepsy for up to 25 days, giving them only a minimal amount of liquid nourishment. The starvation state did help to control seizures, both during the fasting period and in some cases for several months afterward. These results were reported at the 1921 American Medical Association convention. Soon after, a physician at the Mayo Clinic named Russel Wilder realized that starvation itself might not be what was controlling the epilepsy, but rather the ketotic state induced by starvation. Wilder tried an intervention of feeding epileptic children a diet high in fat and low in carbohydrates and found that it was just as effective as starvation in reducing seizure burden. The ketogenic diet was born.
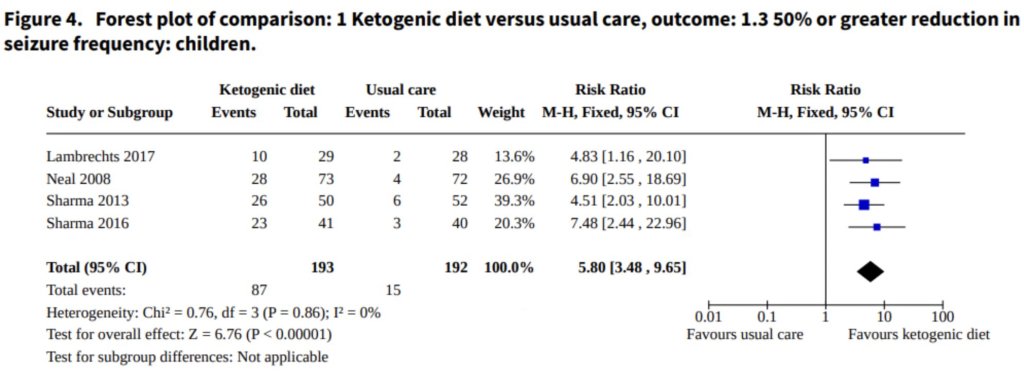
The first formal trial was a 1924 study, also at the Mayo Clinic. Seventeen epileptic patients were treated with a ketogenic diet; 10 became seizure-free. It was soon clear that the ketogenic diet was more effective at preventing seizures than bromides and phenobarbital, the only antiepileptics available in the early part of the 20th century. Subsequent studies have confirmed that the ketogenic diet works, particularly for reducing the seizure burden in children with epilepsy. A 2020 Cochrane review found that the preponderance of evidence shows that a ketogenic diet can significantly benefit the seizure burden in kids with epilepsy. This intervention is still used for difficult-to-control epilepsy if seizure burden persists despite appropriate anticonvulsant therapy. Thankfully, contemporary medical options have advanced beyond phenobarbital and bromides, making the ketogenic diet needed less often than in generations past.
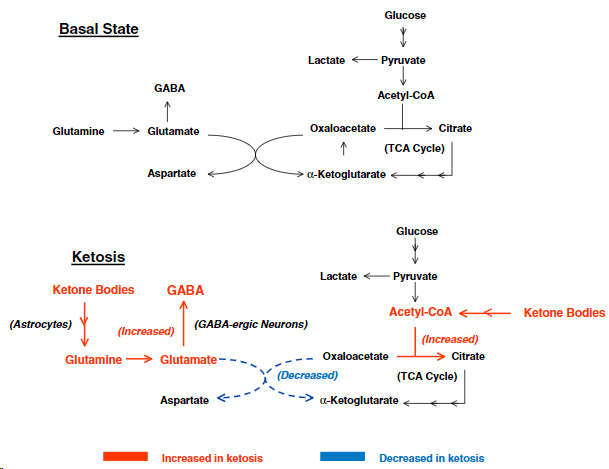
There are three main mechanisms proposed to explain the effect of the ketogenic diet in the prevention of seizures. The first is the GABA shunt. GABA (gamma-aminobutyric acid) is the main inhibitory neurotransmitter in the central nervous system. Ketones are converted in the brain to both glutamine and acetyl-CoA with glutamine further converted to glutamate and then GABA. The high level of brain ketones leads to an increase in seizure-suppressing GABA. What’s more, acetyl-CoA helps drive the glutamate-to-GABA conversion reaction forward even more strongly, and in effect shunts ketones into becoming GABA. This is why this mechanism is named the GABA shunt.
The second proposed mechanism is the metabolic hypothesis. This relates to the notion that decreasing glucose-based metabolism in the brain may have anticonvulsant effects. Supporting this is animal data showing the anticonvulsant effects of avoiding glucose-based brain metabolism. In a 2006 study in Nature Neuroscience, researchers reported that giving rats with temporal lobe epilepsy a compound that inhibits glycolysis (2-Deoxy-D-Glucose) protected them against seizures. Because glycolysis is dependent on glucose to function, blocking glycolysis effectively blocks glucose-based metabolism in favor of ketone production.
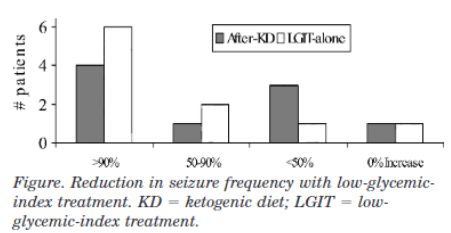
A small clinical trial from 2005 looked at using a low glycemic index diet as an alternative to the ketogenic diet in intractable epilepsy patients. In this situation, carbohydrate intake was more liberalized but restricted to foods that don’t significantly raise blood glucose. Twenty patients were placed on a low glycemic index diet and the majority experienced a reduction in seizure burden; 10 patients had a 90% or more reduction in seizure frequency. This supports the hypothesis that decreasing glucose-based metabolism is contributory to how the ketogenic diet works, since these patients weren’t technically on a ketogenic diet.
The mechanistic basis for the metabolic hypothesis relates to the impacts of slow versus fast neuronal cellular fuel. If one thinks of seizures as a fast-moving electric storm in the brain, it follows that the metabolic fuel need would be high. Glucose provides this fast cellular fuel as it can get rapidly metabolized by glycolysis, generating ATP. Ketones can only be metabolized via the Krebs cycle, a far slower metabolic process. The metabolic hypothesis proposes that neurons receive adequate ATP from ketones, but not as quickly as with glucose. Ketones therefore are a slower cellular fuel source and perhaps less likely to support a seizure.
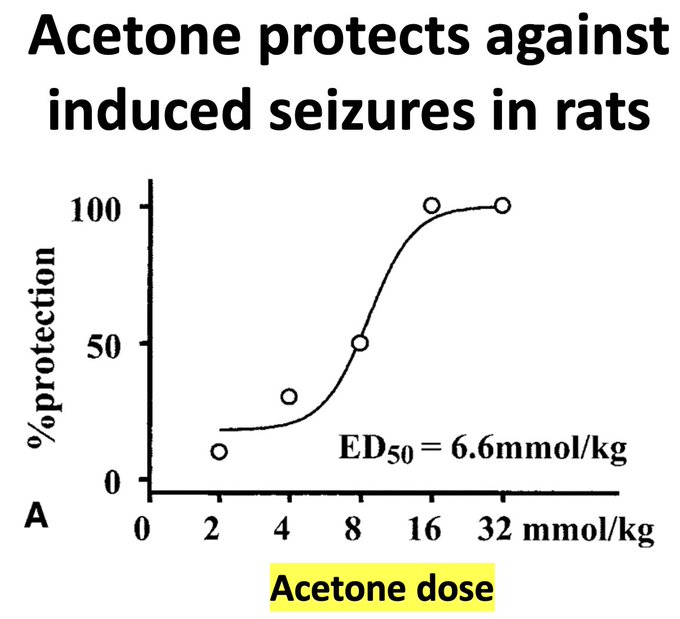
The final explanation is known as the acetone hypothesis. Although ketogenic diets produce acetoacetate, acetone, and beta-hydroxybutyrate, only acetone has direct evidence of anticonvulsant properties. This may be because it crosses the blood-brain barrier more easily than the other types of ketones. A 2003 experiment in rats showed that acetone injection into the peritoneum was protective against multiple different types of induced seizures, with a dose-response relationship: the more acetone the rats received, the more they were protected from seizures. This suggests that acetone, or perhaps a metabolite of it, is a prime component of how the ketogenic diet helps suppress epileptic seizures.
Take Home Points
- Ketogenic diets can be an effective intervention in addition to anti-seizure medications in refractory epilepsy
- The proposed mechanisms include the metabolic hypothesis, the acetone hypothesis, and GABA shunting
- As far back as 500 BC in ancient Greece, it’s been observed that fasting can help prevent seizures; so using ketones as dietary therapy in epilepsy is actually quite ancient
Link to Related Tweetorials
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (0.5 hours), Non-Physician Attendance (0.5 hours), or ABIM MOC Part 2 (0.5 hours).
Listen to the episode
https://directory.libsyn.com/episode/index/id/28367726
Credits & Citation
◾️Episode written by Avi Cooper
◾️ Show notes written by Tony Breu, Giancarlo Buonomo, and Avi Cooper
◾️Audio edited by Clair Morgan of nodderly.com
Cooper AZ, Abrams HR, Breu AC. Kurious Keto. The Curious Clinicians Podcast. October 19, 2023.
