

Each specialty has expertise in a set of symptoms. For a pulmonologist like Avi, that might be undifferentiated dyspnea. For a future hematologist like Hannah, that might be easy bruising. There are some symptoms whose causes span so many diseases and systems that they can’t be owned just by the subspecialists but instead should be “owned” by general internists. Edema is one of them.
For this episode, we discussed the mechanism of edema in nephrotic syndrome. And this meant a reminder about the components of the Starling Equation.

It’s gotta be the albumin
The explanation most often heard on rounds is that the low serum albumin seen in nephrotic syndrome leads to low oncotic pressure which, in tern, leads to edema.
There are a few problems with this explanation.
First, we see lots of patients with albumin levels in the range seen in nephrotic syndrome. These include patients with acute and chronic illnesses. These patients do not typically manifest with generalized edema. Certainly not to the extent seen in some patient with nephrotic syndrome.
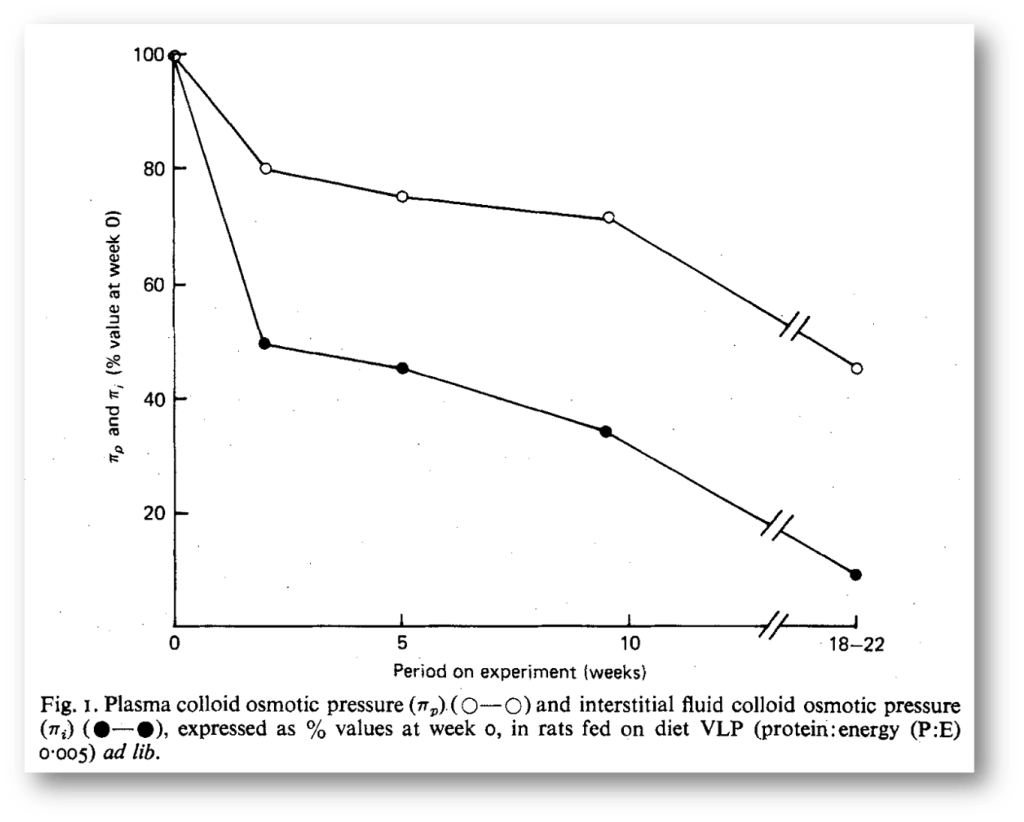
Second, in rats fed a low-protein diet, the interstitial oncotic pressure falls in proportion to the capillary oncotic pressure. This means that the gradient is unchanged and edema does not typically form. This also occurs in nephrotic syndrome.
Lastly, congenital an-albuminemia doesn’t typically manifest with edema. In one series, 50% were asymptomatic and only a third had edema on exam. Example: 21-year-old male with no symptoms and an albumin of 0.
This is not to suggest that hypoalbuminemia plays no role in nephrotic syndrome. It likely does, particularly when the decrease in serum albumin occurs rapidly or if it is severe. For example, with minimal change disease, you might see a rapid decrease to <1. In these cases, the low albumin surely plays a role. But for many patients, particularly adults, oncotic pressure isn’t the key factor in Starlings equation.
Top two contenders
The two leading alternate explanations both rely on increased capillary hydrostatic pressure to explain edema. More specifically, sodium retention leading to increased capillary hydrostatic pressure.
The underfill hypothesis states that even if low albumin seen in nephrotic syndrome doesn’t lead directly to edema it does result in movement of fluid into the interstitial space. This reduces effective circulating volume resulting in activation of the renin-angiotensin-aldosterone sysystem (RAAS) and sodium retention.
The simplest piece of evidence favoring the underfill hypothesis is that some patients with nephrotic syndrome have elevated renin and aldo levels. But not all patients wuth nephrotic syndrome meet this profile.
If there’s underfill, there must be overfill
To pair it with the underfill hypothesis there is – unsurprisingly – the overfill hypothesis. It states that the kidneys are sodium avid not because they are seeing less effective circulating volume but instead because the mechanisms of sodium retention are turned on independently of RAAS.
To understand why this might be, recall that increased glomerular filtration of proteins is key in nephrotic syndrome. We focus on albumin but many other proteins are filtered. This explains the hypercoagulable and immunodeficiency states seen with nephrotic syndrome.
For edema, the increased filtration of serine proteases may be the key. One of the serine proteases that has gotten a lot of attention is plasmin, whose precursor – plasminogen – is found in nephrotic urine.
Plasmin can activate ENaC via proteolytic cleavage of the gamma chain. If ENaC is constitutively active, the kidneys will retain sodium in the absence of RAAS telling them to.

In support of this hypothesis are studies of an animal model of nephrotic syndrome in which mice treated with the serine protease inhibitor aprotinin normalized urinary serine protease activity and prevented sodium retention.
This doesn’t prove plasmin is the key protease. In fact, other proteases, including cathepsin-B, have also been reported to increase ENaC activity in experimental nephrotic syndrome. Independent of which protease is leading to ENaC activation, there is good evidence that ENaC is activated.
Amiloride to the rescue?
Based on the mechanism described above, it should be of no surprise that amiloride has been examined as a potential remedy for the edema of nephrotic syndrome. There are animal studies showing that it reduces sodium retention in nephrotic syndrome. And there are case reports of humans who had diuretics resistant edema who responded well to amiloride. That said, there isn’t enough data to suggest its routine use in patients with nephrotic syndrome. As mentioned throughout, the edema is multifactorial and even if overill from ENaC is the key in some patients, it’s not the only factor and, for some, it may not be the primary driver.
Take Home Points
- Although patients with nephrotic syndrome have hypoalbuminemia, low plasma oncotic pressure isn’t the main driver of edema
- Low plasma albumin may lead to a degree of volume depletion and resulting RAAS-mediated sodium retention. This is called the underfill hypothesis.
- Another leading theory – the overfill hypothesis – states that filtered serine proteases activate ENaC leading to RAAS-independent sodium retention and edema
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (1.00 hours), Non-Physician Attendance (1.00 hours), or ABIM MOC Part 2 (1.00 hours).
Listen to the episode
https://oembed.libsyn.com/embed?item_id=20028629
Credits & Citation
◾️Episode and show notes written by Tony Breu
◾️Audio edited by Clair Morgan of nodderly.com
Breu AC, Cooper AZ, Abrams HR. Why does nephrotic syndrome cause edema? The Curious Clinicians Podcast. August 4, 2021
Image credit: https://www.everydayhealth.com/congestive-heart-failure/edema/
Related tweetorial: https://x.com/tony_breu/status/1014594717034713090
