

The “intern question” for this episode resulted from one of Hannah’s experiences on the wards. She cared for a patient who reported a symptom that was new to her. It was new to all of us. This is a bit unsurprising as it has a relatively limited body of available literature, having been first described in 2013. Despite this, its presence helped Hannah identify a potential diagnosis and let her ponder cardiac physiology. We’ll do the same here.
The symptom: bendopnea
The question: What the heck is it?
What is bendopnea?
Benopnea is shortness of breath experienced during the first 30 seconds after bending forward. As one might predict, it was first described in patients who were dyspneic with tying their shoes! Not all papers call it benopnea. In fact, the first report we found (a case series including 3 patients with heart failure and 5 office staff members) called it “flexo-dyspnea”.
In the first large study, 102 patients with an ejection fraction of <40% who were undergoing right heart catheterization were queried about benopnea. Investigators timed the duration to the onset of shortness of breath and any subject who reported dyspnea within 30 second of bending was classified as having bendopnea. In 46 of the subjects, pressures were also measured when bending forward, as if they were tying their shoes.
What did they find? Benopnea was present in 28% (29/102) of the subjects. Those with benopnea had higher supine pulmonary capillary wedge pressures (23 mmHg versus 19 mmHg). And although there was no difference in the cardiac index between the two groups, patients with bendopnea were more likely to be “cold and wet” (i.e., high pulmonary capillary wedge pressure and low cardiac index).
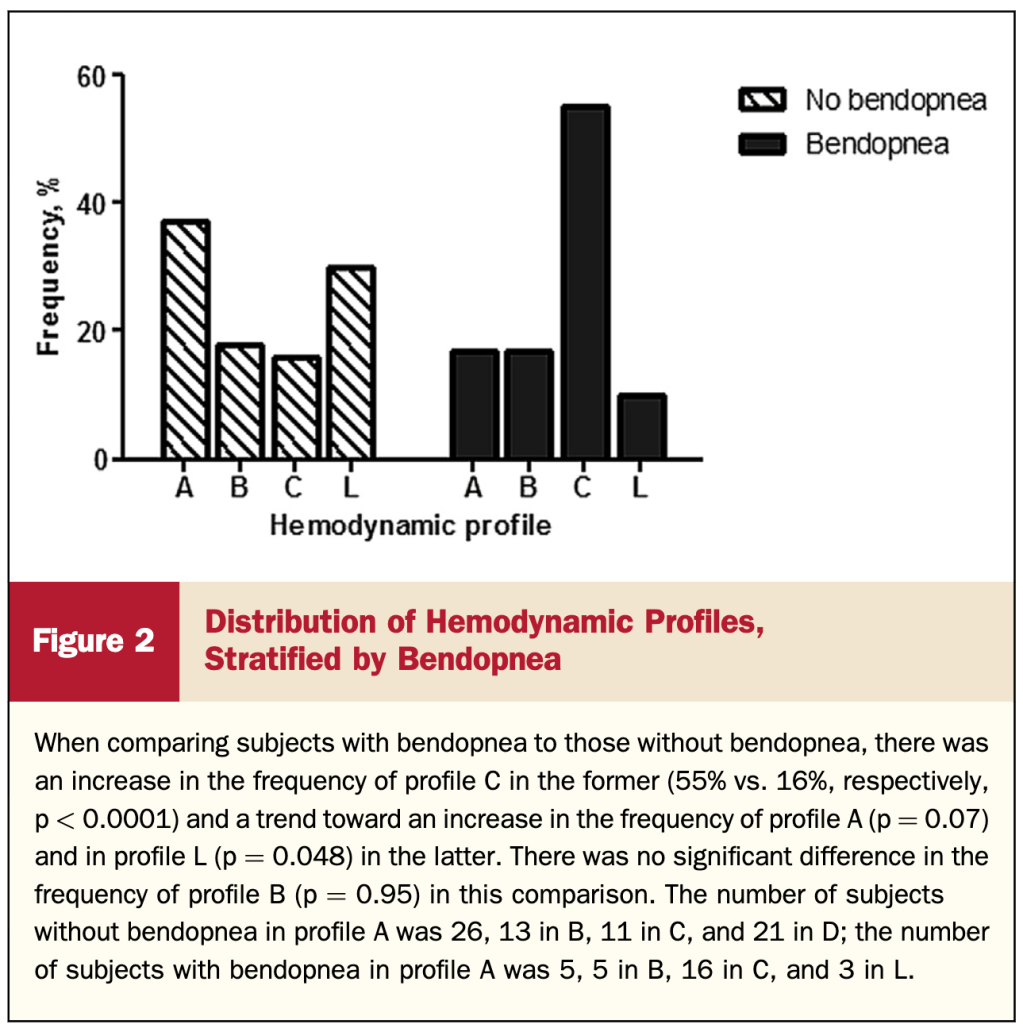
Of those who had hemodynamic monitoring during bending, 35% (16/46) reported benopnea. Both groups had an increase in pulmonary capillary wedge pressure with bending. Interestingly, there was no difference in the amount of increase between the groups.
So it appears that benopnea is a marker of higher filling pressures at rest (as evidenced by the higher supine pulmonary capillary wedge pressures). Provocation with bending forward leads to a similar increase in pressures in those with and without benopnea, but the latter may reach a “threshold” pressure which results in dyspnea.
What’s the significance?
Benopnea is present in 7% of the general population, 15-20% of those with compensated heart failure, and 48% with decompensated heart failure. So it appears that benopnea tracks well with heart failure severity.
In fact, the odds ratio for heart failure was similar for benopnea (2.6) and a more classic sign of heart failure, paroxysmal nocturnal dyspnea (2.4). And benopnea is associated with greater 6 month mortality and readmissions.
One study even evaluated the evolution of bendopnea during admissions in patients with decompensated heart failure. Among the 60 patients who had bendopnea on the day of presentation ,40 showed improvement in this symptom at the time of discharge.
Specific for heart failure?
It is important to note that conditions other than heart failure have been associated with benodpenia. Examples include allergic bronchopulmonary aspergillosis, pulmonary hypertension and obstructive sleep apnea.
Take Home Points
- Bendopnea is a symptom associated with elevated left venctricular filling pressures.
- Although studied most in heart failure, benopnea can be seen in other conditions.
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (1.00 hours), Non-Physician Attendance (1.00 hours), or ABIM MOC Part 2 (1.00 hours).
Listen to the episode
Credits & Citation
◾️Episode written by Hannah Abrams
◾️Show notes written by Tony Breu and Hannah Abrams
◾️Audio edited by Clair Morgan of nodderly.com
Abrams HR, Breu AC, Cooper AZ. Why does “bendopnea” occur? The Curious Clinicians Podcast. April 14, 2021
Image credit: https://en.wikipedia.org/wiki/Bendopnea

Please decide whether to write “bendopnea” or “benopnea.”
LikeLike