
This episode of the podcast was inspired by a patient Hannah cared for. The patient was found to have septic pulmonary embolism (SPE). On rounds, Hannah’s fellow offered an explanation. Hannah was inspired by this and dug into the topic a bit more.
Septic vs Bland Pulmonary Embolism
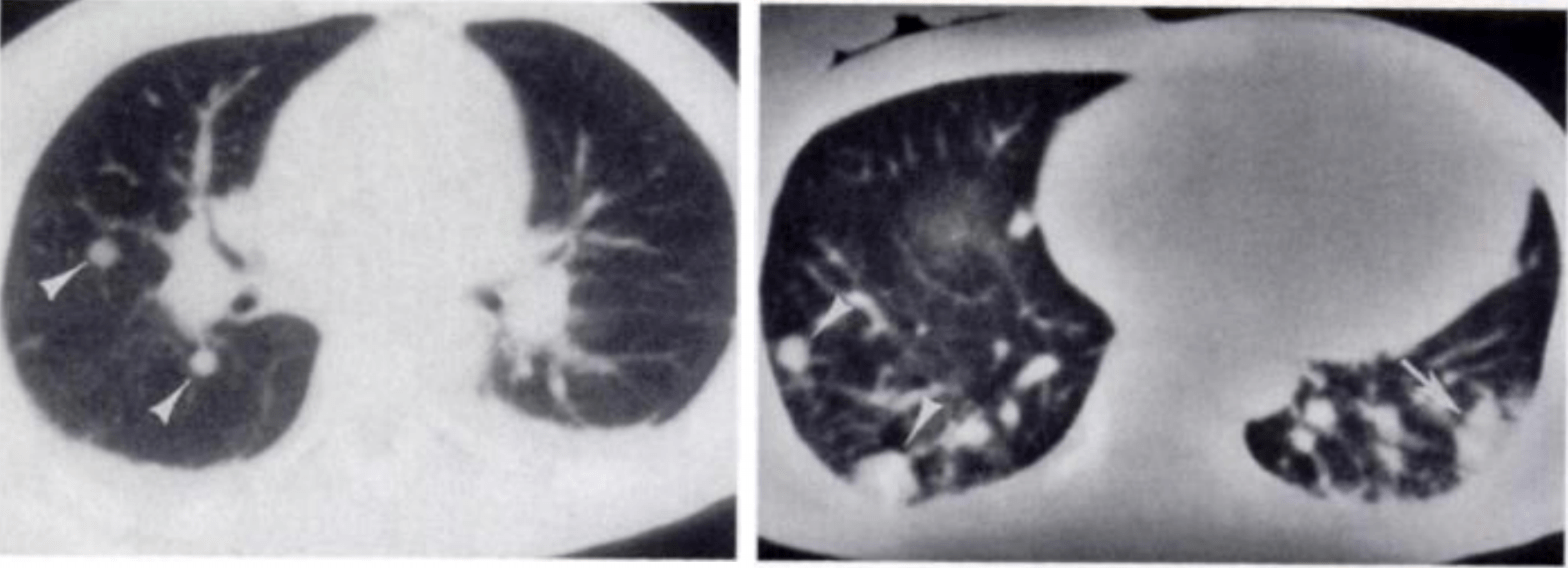
A septic pulmonary embolus is a clot made up of microorganisms in a fibrin matrix that mobilizes from some an infectious nidus – often tricuspid valve endocarditis – and lodges in the pulmonary vasculature. What we see, usually on CT of the chest, is largely the reaction and infarction around these clots. They are classically seen more common in the periphery of the lung, often abutting the pleura, and predominantly found in the bases of the lung.
Non-septic (i.e., “bland”) pulmonary emboli don’t usually form nodules, cavitate, or result in permanent parenchymal damage.
Why the periphery…
Unlike SPE – which typically occur in the periphery of the lungs – bland pulmonary emboli do not limit themselves to the peripheral vasculature. The first and perhaps most obvious explanation for this difference is size. Given that SPE originate from vegetations on the tricuspid or pulmonic valves, they tend to be smaller. As a result, they travel further into smaller vessels at the periphery of the pulmonary vasculature.
But beyond their location, SPE lead to more descruption. Two hypotheses might explain this:
- Most proximal pulmonary vasculature receives collateral flow from the bronchial circulation. Therefore larger and more central clots would likely not demonstrate the same parenchymal infarction and cavitation.
- There is a marked inflammatory response to the organisms within SPE. Pathologically, these emboli are associated with surrounding acute inflammation and go on to form micro-abscesses. Radiologically, one study found that these peripheral wedge shaped infarcts had greater peripheral contrast enhancement along the margins of the lesions, likely representing increased vascularization in response to infection, and therefore a greater propensity to bleed into the parenchyma.
…and the bases?
SPE have a propensity to travel toward the bases of the lungs. In one study characterizing radiographic patterns, 61% of patients had a basilar-predominant pattern. Hannah’s fellow offered an interesting hypothesis: she pointed out that the bases of the lung receive the greatest circulation (or Q if you’re thinking about West zones), and therefore any flow-dependent process, like the movement of small clots, should also predominate at the bases!
GNR vs GPCs
One study examined the radiographic features of SPE and compared the findings in infections due to gram negative rods (GNRs) and gram positive cocci (GPCs). Septic pulmonary emboli associated with GPCs were larger, more likely to form cavities, and were more associated with wedge-shaped infarcts. Septic pulmonary emboli associated with GNRs were smaller, better-demarcated, and associated with local hemorrhage (demonstrated by presence of a “halo sign”). The authors hypothesize that this may be because of the vascular effects of endotoxin for gram negatives.
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (1.00 hours), Non-Physician Attendance (1.00 hours), or ABIM MOC Part 2 (1.00 hours).
Listen to the episode
Credits & Citation
◾️Episode written by Hannah Abrams
◾️Audio edited by Hannah Abrams and Clair Morgan of nodderly.com
◾️Show notes by Tony Breu and Hannah Abrams
Abrams HR, Cooper AZ, Breu AC. Why do septic pulmonary emboli occur in the periphery and bases of the lungs? The Curious Clinicians Podcast. November 25, 2020. https://curiousclinicians.com/2020/11/25/episode-14-septic-pulmonary-embolism/(opens in a new tab)
Image credit: Kuhlman JE, Fishman EK, Teigen C. Pulmonary septic emboli: diagnosis with CT. Radiology. 1990;174(1):211-213.
