

Many of you know that azithromycin is often used as part of the treatment of acute exacerbations of chronic obstructive pulmonary disease (COPD). And this is done even when there is no evidence of a bacterial infection. That means there are two possible explanations: (1) it’s just assumed that there is a bacterial infection there, even though we’re unable to diagnose it or (2) we’re using azithromycin (and really other macrolides) for some other purpose.
For this episode of the podcast, we examined explanation #2. This was also covered in a Tweetorial Tony posted on April 17, 2020. Here’s a link:
When/why were macrolides first used for anti-inflammatory reasons?
Before getting into the mechanisms involved, it’s worth discussing some of the history behind macrolide use as anti-inflammatories.
In the 1960s, the use of triacetyloleandomycin and erythromycin in steroid-dependent patients with asthma enabled clinicians to significantly decrease steroid doses without worsening airway function. And, infection could not be detected with any greater certainty in patients who responded than in those who did not. This suggested a property of macrolides beyond their ability to kill bacterial.
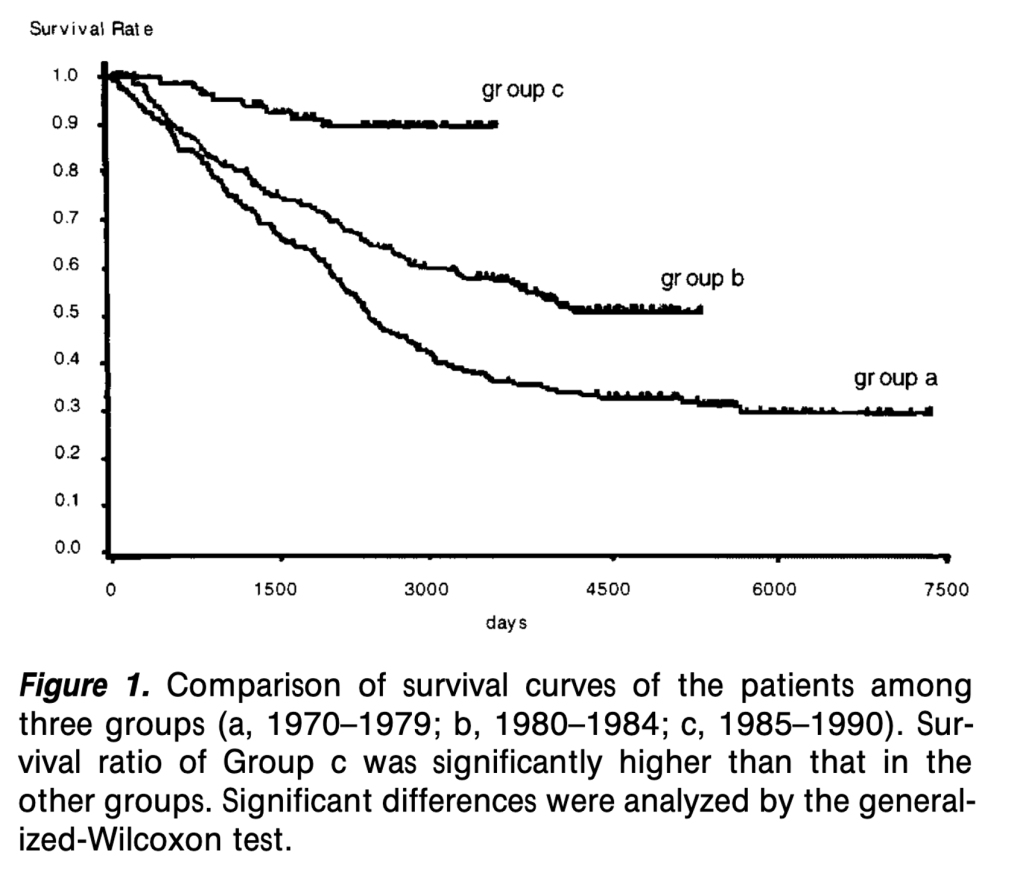
But it wasn’t until the 1980s that it became clear that macrolides were doing something immunomodulatory. Patients with panbronchiolitis (a form of inflammatory bronchiolitis which presents with a progressive decline in lung function) significantly improved 10-year survival rates after treatment with erythromycin. 90% for those on the macrolide versus 40% for those not receiving it.
How do macrolides do this?
There are two broad ways that macrolides act as anti-inflammatories. One is pathogen directed. The other is immune-system directed.
(1) To understand the pathogen-directed mechanism, it is important to remember the mechanism of action of macrolides: they decrease protein synthesis via inhibition of 50S large ribosomal subunit. Their antimicrobial activity results because the bacteria can’t make the cell wall.
But, this mechanism also means other proinflammatory protein toxins and virulence factors such as bacterial adhesins and biofilm aren’t produced. This can occur at sub-minimal MICs, meaning that the macrolide doesn’t have to be given at doses that typically inhibit bacterial growth for this effect to be seen. And, it also occurs with organisms typically resistant to macrolides (e.g., pseudomonas). This is one reason why patients with cystic fibrosis are treated with macrolides.
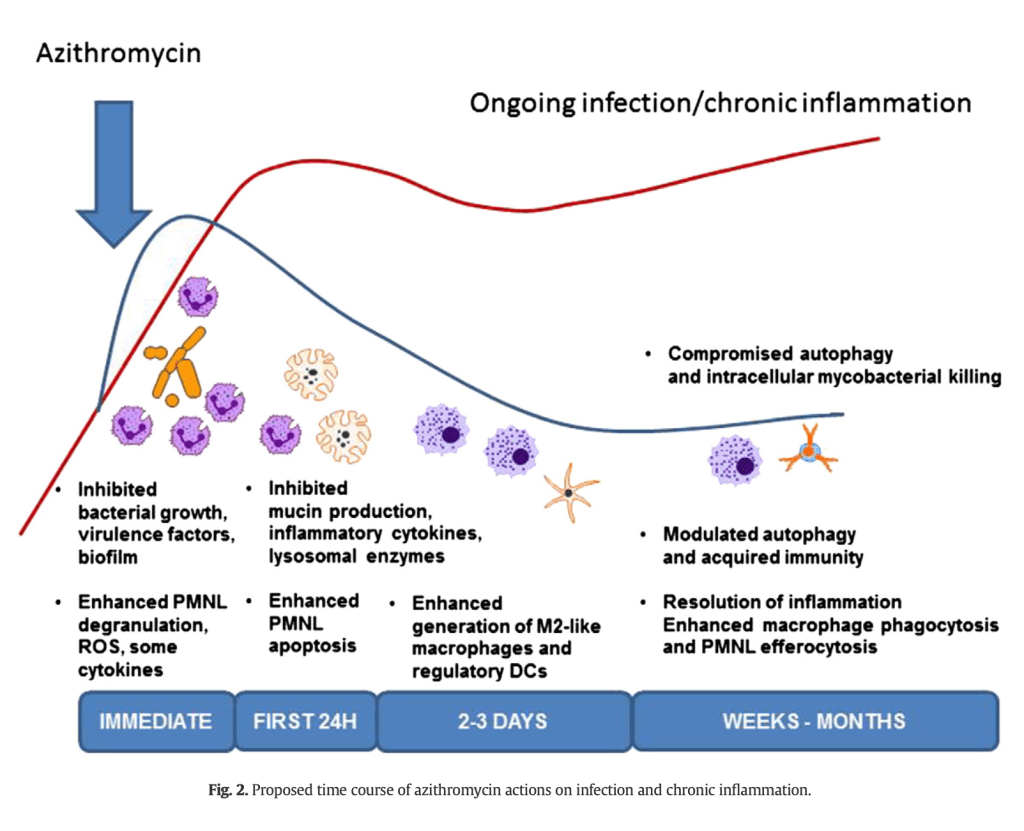
(2) The immunomodulatory effects of macrolides are complex. They probably have a biphasic immunomodulatory effect (see picture below). There is initial neutrophil stimulation, shown by degranulation and enhanced oxidative response. This early phase also includes a fall in chemokine and cytokine concentrations that persist. Later, there is a down-regulation of the oxidative burst and an increase in apoptosis of neutrophils.
Cytokines!
Macrolides affect many types of cytokine and chemokines. One of the major targets is IL-8, one of the cysteine-X-cysteine (CXC) chemokines that is a potent neutrophil chemoattractant. That means it brings neutrophils to sites where they are needed. Or, sometimes to places where we may not want them. For conditions like COPD, IL-8 helps to localize PMNs to the lung. Erythromycin inhibits IL-8 release in the airways of patients with chronic airway disease and clarithromycin decreases in IL-8 and TNF-alpha levels (see picture below).

If we go back to the mechanism of action, remember that macrolides accumulate inside cells, including immune cells, at concentrations 90-350x higher than in serum. And they accumulate inside for at least 28 days. In fact, the intensity of anti-inflammatory activity correlates with cellular accumulation. One study found that IL-6 and prostaglandin E2 suppression were highest when the cellular concentration of the macrolide (or other compound) was highest.
Inside the cells, macrolides inhibit transcription factor nuclear factor-kappa B. This probably results in the reduction in IL-8.
Do we even need azithromycin?
For patients with acute exacerbations of COPD, one might wonder why we use a macrolide if we’re already administering prednisone. Isn’t the steroid enough of an anti-inflammatory that the azithromycin is unnecessary?
But, it turns out steroids only have a modest effect on airway inflammation in COPD. The reason: there is reduced histone deacetylase activity in COPD patients.
Why is this relevant? Remember that DNA is wound around histones. When the body requires an inflammatory response, the relevant histones undergo acetylation, leading to increased expression of the key gene. Steroids typically reverse this process by deacetylating those histones. But, in COPD, this activity is decreased and steroids just don’t work as well. And to tie it all together, macrolides may increase histone deacetylase, restoring the anti-inflammatory effect of steroids!
What about other conditions?
Given the inti-inflammatory nature of macrolides, it should come as little surprise that they have been trialed in conditions other than those mentioned above. Some examples:
- There is some evidence that macrolides have direct antiviral activity. For example, azithromycin reduced Zika proliferation in glial cells. There is also in vitro and in vivo data showing efficacy of macrolides in rhinovirus, respiratory syncytial virus, and influenza virus. There is even a randomized control trial showing azithromycin reduces severe lower respiratory tract infections in kids. These infections are typically viral.
- One randomized control trial examined the effects of clarithromycin in patients undergoing mastectomy. Patients treated with clarithromycin had lower temperatures, reduced the intensity and duration of postoperative pain, and increased the range of motion of the involved shoulder.
- Azithromycin has even been tested in experimental mouse models of pancreatitis, though with negative results.
Take home points
- Macrolides decrease toxin production and can do this for bacteria they don’t typically target.
- IL-8 is a chemokine that recruits neutrophils
- Macrolides decrease IL-8 levels in the lung
- This may lead to decreased inflammation
- There are many other anti-inflammatory and immunomodulatory effects of macrolides!
Learning Objectives
- Explore how macrolides – including azithromycin – act as anti-inflammatory agents.
- Review the mechanism of action of macrolides and how this informs their anti-inflammatory effects.
- Identify potential uses of macrolides given their anti-inflammatory properties.
CME/MOC
We are excited that The Curious Clinicians have partnered with VCU Health Continuing Education to offer continuing education credits for physicians and other healthcare professionals. Visit VCU Health for more information.
Listen to the episode
Credits & Citation
◾️Episode written by Tony Breu
◾️Episode audio edited by Clair Morgan of Nodderly
◾️Show notes by Tony Breu
Breu AC, Abrams HR, Cooper AZ. Why is azithromycin anti-inflammatory? The Curious Clinicians Podcast. August 5, 2020. https://curiousclinicians.com/2020/08/05/episode-6-why-is-azithromycin-anti-inflammatory/
Opening image source: https://www.youtube.com/watch?v=o0lqQwpNBZg

Excelent
LikeLike