

For this episode we discuss a tweetorial Tony posted on September 4, 2018. Here’s a link to the full thread:
A bit of history
In addition to the content covered in the tweetorial, we discussed some history. In 1865, Armand Trousseau, a French physician, was one of the first to describe an association between thrombosis and cancer [he also made an appearance in Episode 1]. The association had actually been reported decades earlier (in 1823) by Jean Baptiste Bouillaud, another French physician. Perhaps because of the irony of Trousseau diagnosing the condition on himself and dying from it in 1867, the condition was later called Trousseau syndrome.
Epidemiology of VTE and cancer
How strongly is cancer associated with the risk of venous thromboembolism (VTE)? The case-control study mentioned in the tweetorial found odds ratios (OR) between 4.1 and 6.5, depending on whether patients were receiving chemotherapy. This is higher than some risk factors (e.g., varicose veins) but lower than others (e.g., surgery or trauma).
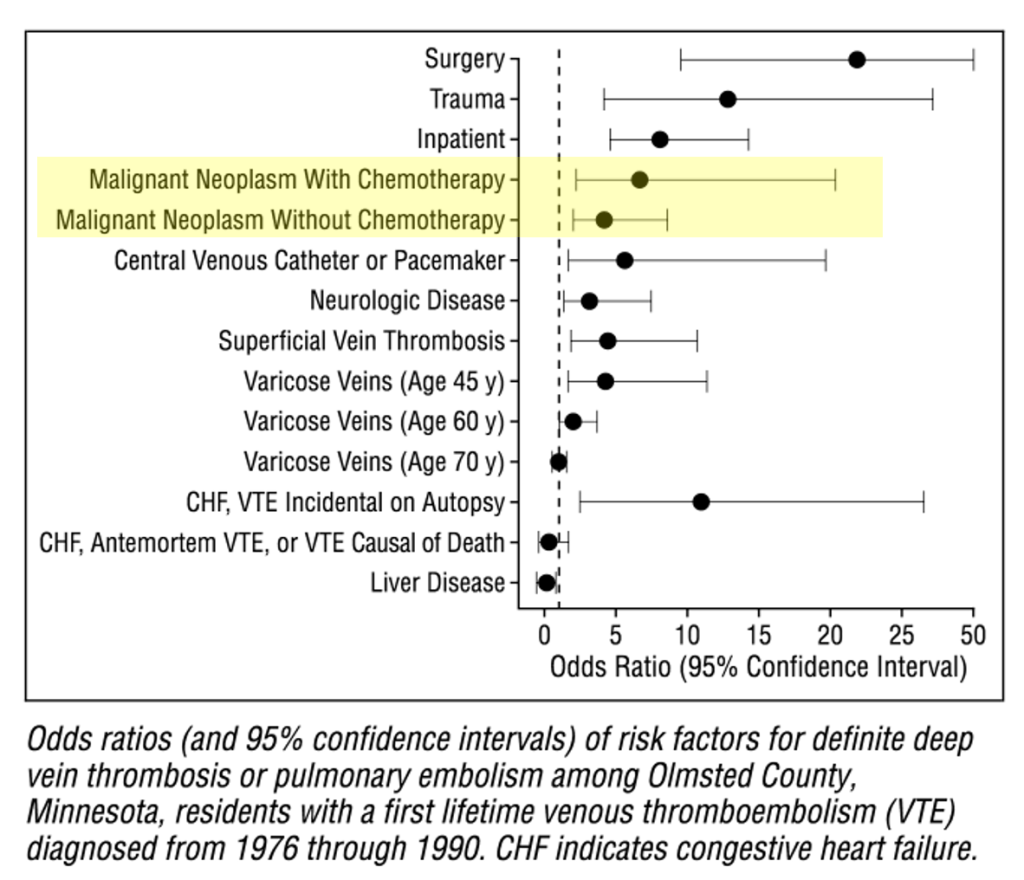
Additional studies on the epidemiology of venous thromboembolism and cancer were discussed:
- A more recent cohort found an OR of 6.7.
- The absolute risk for a patient with cancer is between 1-8% per year. This is much higher than the rates in the general population: 1 per 10,000 annually before the fourth decade of life, rising rapidly after age 45 years, and approaching 5–6 per 1000 annually by age 80.
- Some cancers (e.g., pancreatic and brain) are more strongly associated.
Mechanism of VTE risk in cancer
The mechanism of thromboembolism in cancer is undoubtably multifactorial and likely involves all three arms of Virchow’s Triad. The tweetorial and this episode of the podcast concentrated on the hypercoagulable state in cancer and the specific role of Tissue Factor (aka Factor 3):
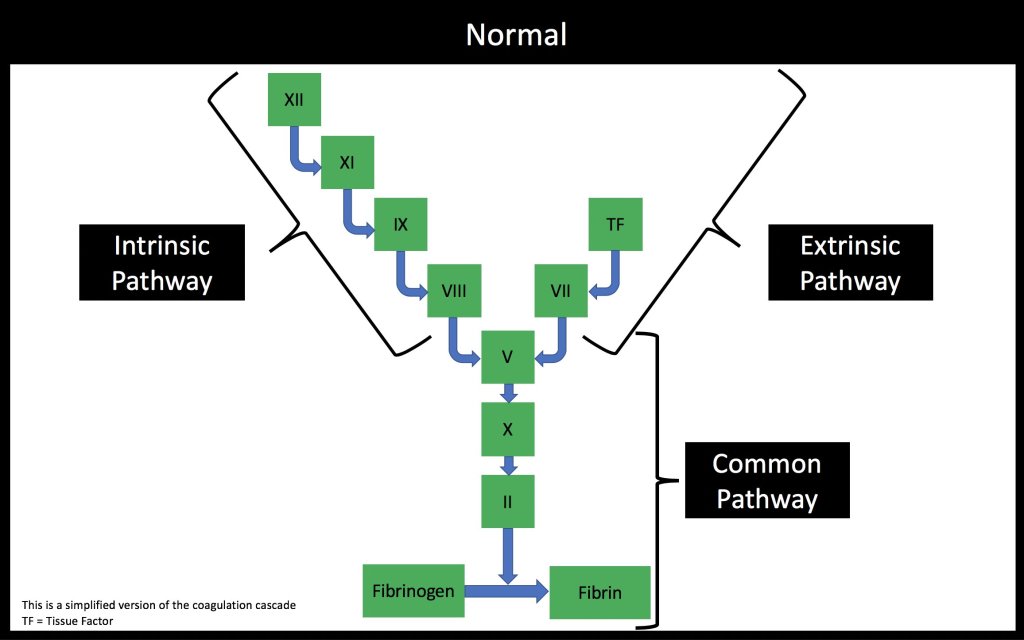
Key features of Tissue Factor:
◾️Expressed in adventitial fibroblasts of the vessel wall
◾️Increased when vessels are injured
◾️Forms a complex with factor VII to activate factor IX and factor X
💥Initiates coagulation
One potential reason why TF may be increased in cancer relates to the inflammatory state. Cancer cells interact with monocytes, resulting in a release of cytokines (e.g., IL-1, IL-6, TNF) which cause endothelial injury and release of TF.
More intriguingly, some tumors show increased expression of TF. This increased expression has been linked to increased rates of VTE. The best example is pancreatic cancer where:
◾️26.3% of those with high TF expression had VTE
◾️4.5% of those low TF expression had VTE
Some cancers produce TF-bearing microparticles that lack the transmembrane domain and are less than a micron in diameter. The presence of these microparticles is associated with VTE with the followeing 1-year incidence:
◾️34.8% if present
◾️0% if absent
What about platelets?
Hannah invoked platelets, to nobody’s surprise. She told us about a few studies that found markers of platelet function (e.g., vWF and p-selectin) are increased in patients with cancer relative to those without. They are also worse in advanced stages with elevated levels associated with increased risk of clotting. As she put it, these studies are sort of like seeing the handprints at the crime scene and knowing platelets were there.
One study did rotational thromboelastometry (ROTEM) on pre- and post- resection blood samples of esophageal cancer patients and found that they were persistently hypercoagulable in clinic (~2 weeks later). Maximum clot firmness, which is a measure of platelet activity, was specifically elevated. In long-term cancer survivors, well after remission for most, vWF is still elevated and both thrombosis & CAD are more common.
Unsuprisingly, there is more to the risk of VTE in cancer than just Tissue Factor or the coagulation cascade.
Does cancer benefit?
There are a couple questions that follows from these observations: why does cancer spend its time making clot? Does it somehow benefit?
Observations and hypotheses were made as far back as 1878 when Theodor Billroth observed tumor cells within thrombus and related this to metastatic formation. Later, it was proposed that fibrin might protect tumor cells from the immune system and facilitate microvascular entrapment needed for metastasis.
Based on these observations, an early RCT showed benefit in patients with small-cell lung cancer, a type of cancer known to have fibrin formation. Median survival was higher in the arm that received warfarin:
◾️50 weeks (warfarin)
◾️24 weeks (control)

Another cool study showed that patients with idiopathic VTE treated with 6 months of anticoag had lower rates of cancer when compared with those treated for 6 weeks: 16% v. 10%. Finally, a Cochrane meta-analysis showed an 8% reduction in mortality at 24 months with use of anticoagulation in patients with cancer and no history of VTE. Whether this reduction is a result of a reduction in VTE or a direct anti-tumor effect is not clear.
Other interesting observations
To close the episode, we discussed a few other conncections:
- Cancer associated is not only associated with increased VTE, it is also associated with another thrombotic condition: nonbacterial thrombotic endocarditis
- A low PTT can be a clue to VTE risk. In one study of non-cancer patients, the OR for VTE in those with a low (i.e., fast) PTT was 2.4. There is less data in patients with cancer though one study did report a correlation with catheter-related VTE.
Take home points
- Cancer is associated with an increased risk of VTE with ORs ~4-7 depending on cancer type, whether chemotherapy is being administered, among other things.
- The ‘hypercoagulable state’ is itself multifactorial, though increased Tissue Factor is a main hypothesis.
- Cancer may be using this to evade immune system and metastasize.
Learning Objectives
- Review the correlation between cancer and risk of venous thromboembolism.
- Outline the multiple ways cancer increases the risk of venous thromboembolism.
- Understand the role of Tissue Factor in normal clotting and the increased risk of venous thromboembolism seen in cancer.
- Apply mechanisms of increased risk of venous thromboembolism in cancer to potential therapeutic interventions.
CME/MOC
We are excited that The Curious Clinicians have partnered with VCU Health Continuing Education to offer continuing education credits for physicians and other healthcare professionals. Visit VCU Health for more information.
Listen to the episode
Credits & Citation
◾️Episode written by Tony Breu
◾️Audio edited by Hannah Abrams
◾️Show notes by Tony Breu
Breu AC, Cooper AZ, Abrams HR. Why is cancer a hypercoagulable state? The Curious Clinicians Podcast. June 10, 2020. https://curiousclinicians.com/2020/06/10/episode-1-why-is-cancer-considered-a-hypercoaguable-state/
Opening image source: https://www.aliem.com/aliemcards-tranexamic-acid/fibrin-clot/
