
Why does an upper GIB increase the BUN/Cr ratio?
The idea that something other than kidney injury might lead to elevations in BUN was first identified in 1912 in infants with cholera. The entity was called extrarenal azotemia. In retrospect, these were likely instances of prerenal azotemia, but the clinicians could not identify renal abnormalities histologically and therefore considered the condition to be outside the kidneys. In 1933, LV Sanguinetti was the first to note that GI bleeding is associated with an elevated BUN. The next two decades were the golden age of experimentation on this question, with dozens of studies done with the goal of identifying the cause.
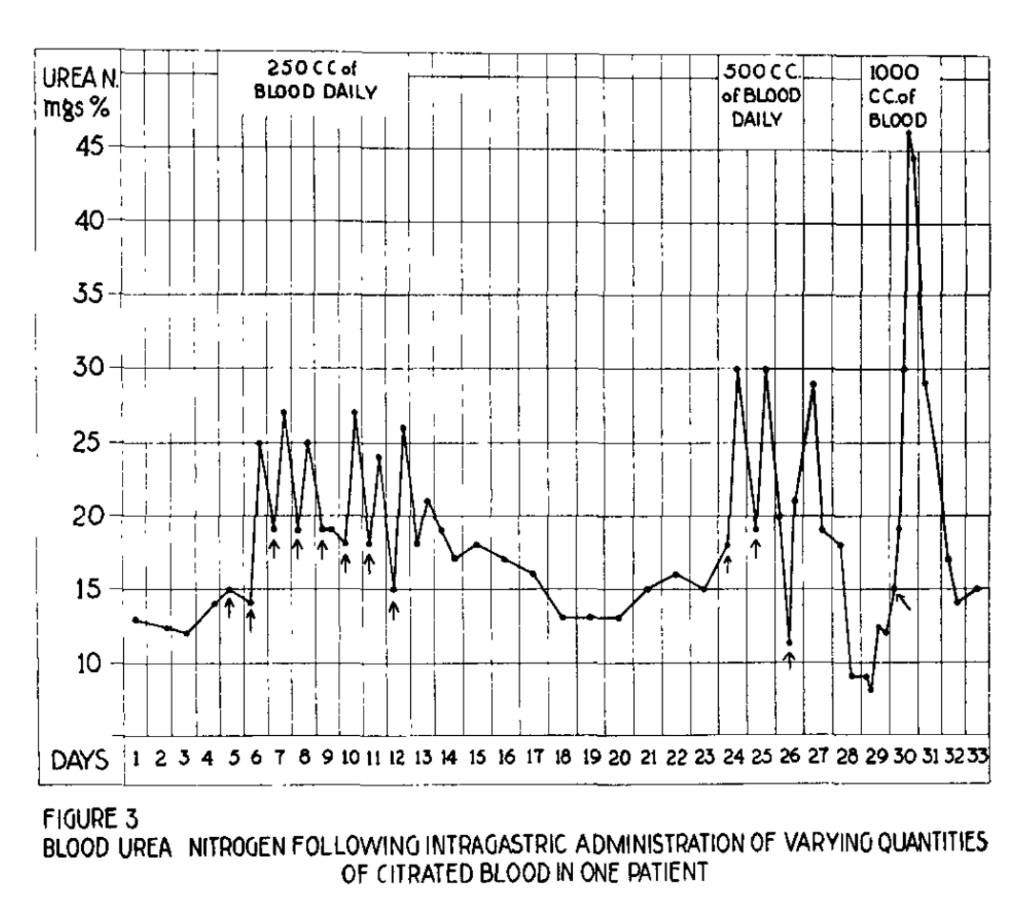
One of the main investigators was Leon Schiff. In 1939 he and three other researchers published a set of experiments in The American Journal of Digestive Diseases. In one experiment, they enrolled 15 participants and fed them blood that was 3 weeks old and, therefore, deemed too old for transfusion. They examined how the BUN changed based on the amount of blood administered and the site of administration.
When 250 mL of blood was administered via an orogastric tube (OG), they saw a very small rise in BUN. As they increased the dose of blood to 500, 1000, and 2000 mL they saw a greater increase in BUN.
Schiff and his colleagues also identified a set of patients who had experienced hematemesis with an increase in their BUN. Once these patients stabilized, they administered 2 liters of blood via the OG tube. When they did, the increase in BUN matched quite well what was seen during their bleed.
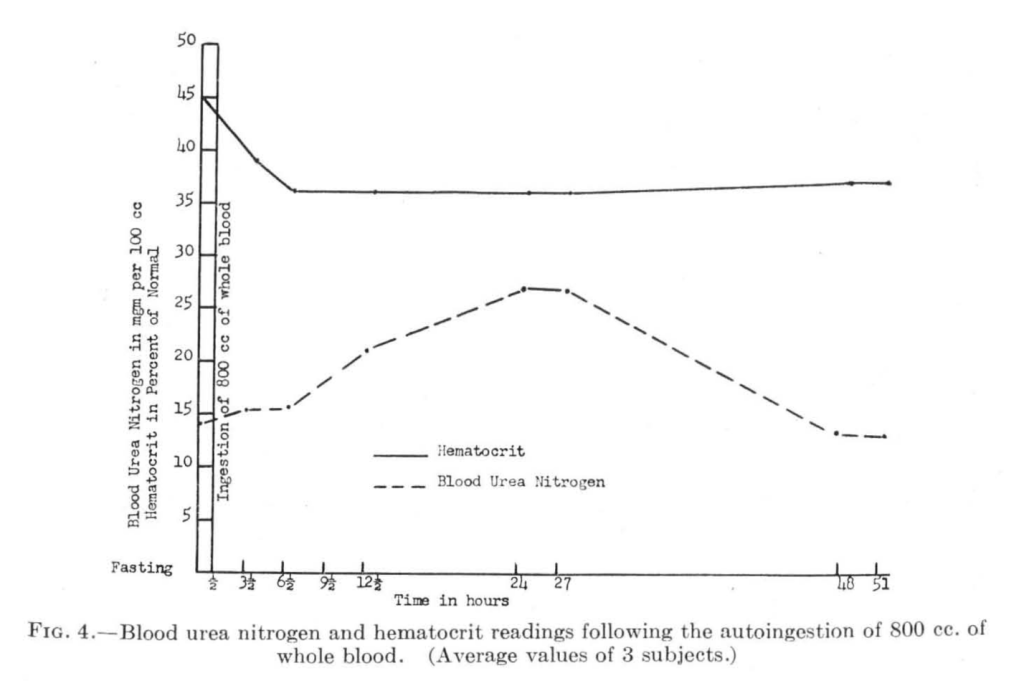
In another study done by Captain IJ Greenblatt of the US Army and published in 1946 the authors and other military officers underwent phlebotomy with 580mL or 800mL of their own blood drawn. They then drank it with 100mL of water over 30 minutes. They were allowed to have peppermint candy, a smoke, and some water during the next few hours, during which their BUN was repeatedly checked. The authors tell us that for the participants, “the psychic trauma was non-existent,” so that’s reassuring.
The BUN did not increase much with 580cc of blood removed and ingested but did increase with 800cc. But the loss of blood didn’t seem to exaggerate the rise seen in Schiff’s or others’ experiments.
These are just two of many many variations on experiments where various amounts of blood were ingested or otherwise placed into the stomach. Most resulted in an increase in BUN, particularly as more blood was administered. But when Schiff et al placed blood into the jejunum or the upper ileum, a smaller rise in BUN was seen. And after colonic administration, no increase in BUN was seen.
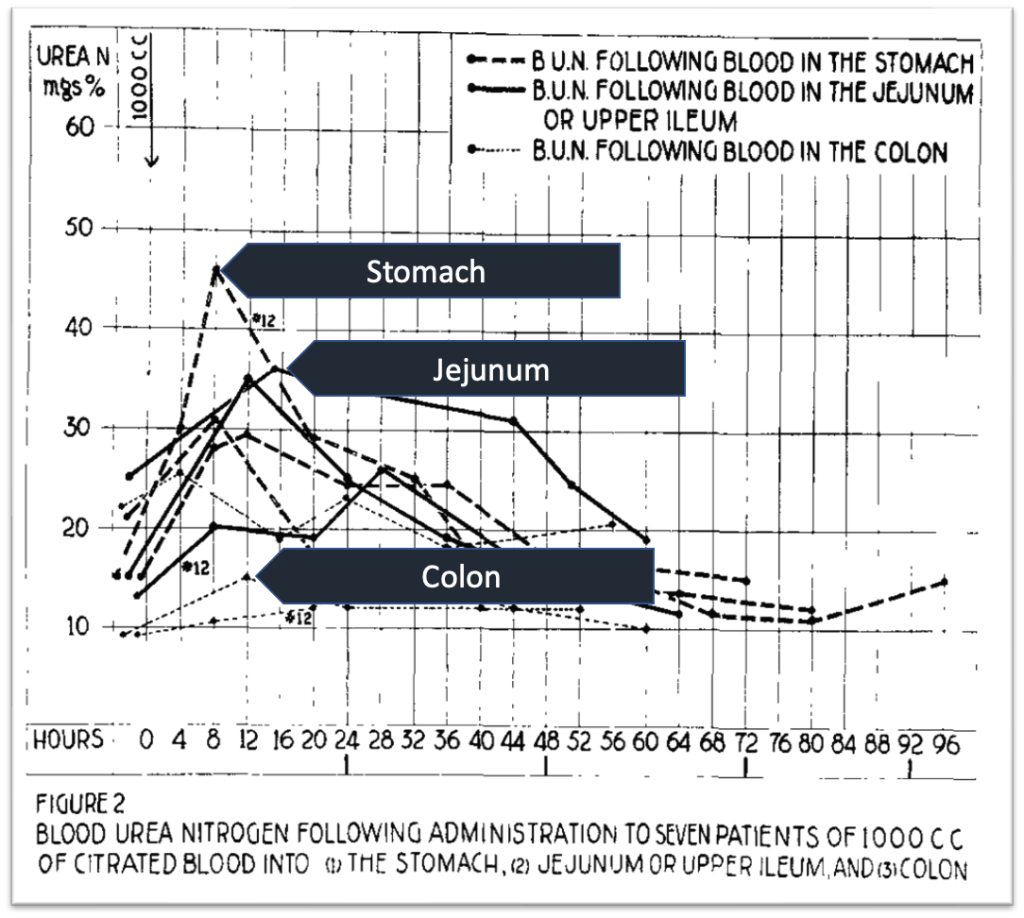
This supports the idea that an increase in BUN/Cr is really a phenomenon of upper GI bleeding.
The question then becomes: what is the mechanism?
The ultimate explanation is surely multifactorial. But, the experiments outlined above support the notion that there is something specific about the placement of blood into the stomach or upper small intestine that leads to these changes. Understanding the full mechanism requires a review of why the body bothers to generate urea in the first place.
Urea is a byproduct of protein metabolism. When proteins are ingested, they are degraded to amino acids by gastric and pancreatic peptidases or by brush-border enzymes. These amino acids are then transported into proximal small intestine enterocytes and then into the blood. If the proximal small intestine is the site of amino acid absorption, this explains why upper GI bleeds are more likely to lead to a rise in BUN.
After the amino acids are absorbed, they are metabolized into nitrogen products and carbon products. The carbon products are either stored or used to generate ATP. The nitrogen products are converted to ammonia. Ammonia is then funneled into the aptly named urea cycle, the end product of which is urea.
We often talk about albumin as being the most common protein in the blood, but that is not quite right. It’s the most plentiful protein in the plasma and serum, but when you look at whole blood, another protein is even more plentiful. Hemoglobin.
Assuming a hemoglobin of 15 g/dL, a one-liter GI bleed contains 5 trillion red blood cells. Each red blood cell contains 260 million molecules of hemoglobin. And each hemoglobin contains 574 amino acids. Do the math, and you get 700 sextillion amino acids in one liter of blood. That’s 7 x 1023 amino acids generated from the hemoglobin.
One of the interesting characteristics of hemoglobin is that it lacks isoleucine, one of the essential amino acids. This means that hemoglobin is considered a protein with low biologic value. Biological value is the proportion of absorbed protein incorporated into the other proteins of the organism’s body. Amino acid content is the main determinant of biological value. Proteins lacking an essential amino acid (e.g., isoleucine) have low biological value.
Some have argued that this characteristic of hemoglobin results in an inability for the body to use metabolized it to make other proteins, as most will require isoleucine. This means that hemoglobin is more likely to generate urea. Tying this thread together is data showing that protein synthesis decreases after a simulated GI bleed. And even cooler, you can mitigate the reduction in protein synthesis if you infuse isoleucine.
Other ingested proteins can also lead to a rise in BUN. If we go back to Leon Schiff’s 1939 study, he also gave participants 1.8 kg of lean beef steaks and monitored BUN afterward. He saw an increase in BUN that matched what was seen in a 2-liter blood meal. Other studies have shown similar results.
But notice that this is a lot of beef protein. A normal-sized steak is about 10 ounces and contains about 70 grams of protein. Schiff gave about 350 grams of protein. That’s the equivalent of 5 steaks. So if one had a 5-steak dinner and had their blood work checked, you might see an increase in their BUN.
The above discussion confirms that the BUN increased in an upper GI bleed. But, in order for the ratio to rise, the creatinine must be less affected. Because creatinine is generated exclusively from the metabolism of muscle protein, ingestion of blood protein won’t affect it. So you get a rise in BUN without a concomitant rise in creatinine. Thus the rise in the ratio.
Take Home Points
- The 1930s were the heyday of “let’s make this person ingest blood” experimentation.
- These data, and those that followed, suggest that absorption of hemoglobin from blood leads to the increase in BUN seen in upper GI bleeds.
- Because creatinine is not affected by the absorption of blood proteins, like hemoglobin, this value does not change. The result is an elevation in the BUN/Cr ratio.
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (0.5 hours), Non-Physician Attendance (0.5 hours), or ABIM MOC Part 2 (0.5 hours).
Listen to the episode
https://directory.libsyn.com/episode/index/id/26740755
Link to associated tweetorial
Credits & Citation
◾️Episode and show notes written by Tony Breu
◾️Audio edited by Clair Morgan of nodderly.com
Breu AC, Cooper AZ, Abrams HR. Blood meal. The Curious Clinicians Podcast. May 3, 2023.
This episode was sponsored by Green Chef!
Image credit: https://en.wikipedia.org/wiki/Hemoglobin

One thought on “Episode 70 – Blood meal”