
Should I consider atrial fibrillation a risk factor for
pulmonary embolism?
Most of us have probably learned that a pulmonary embolism can cause right heart strain and lead to atrial fibrillation. But why can’t the reverse be true? Why isn’t atrial fibrillation considered a risk factor for pulmonary embolism? If the right atria is beating chaotically, why wouldn’t this predispose to the formation of a thrombus and, ultimately, an increased risk of embolization to the pulmonary arteries?
Maybe atrial fibrillation does cause pulmonary embolism.
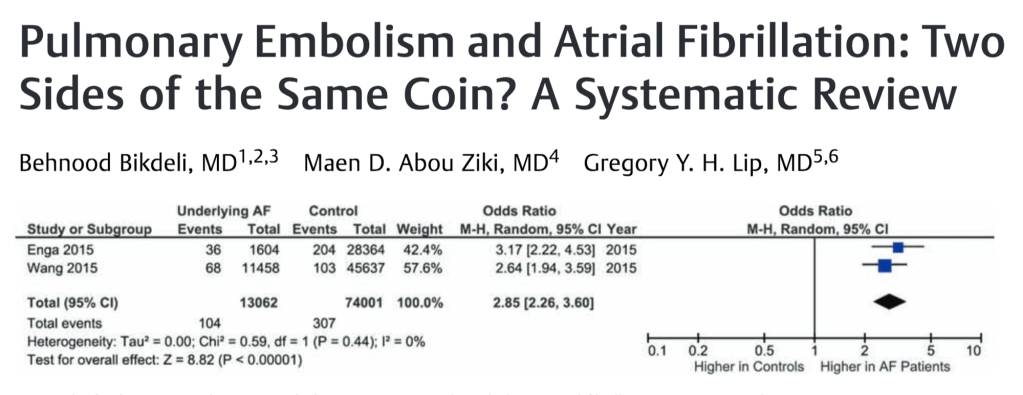
As one can imagine, we only have observational data showing the connection between these two conditions. Nobody is doing a study where they randomly allocate some participants to induced atrial fibrillation (AF) to see if that leads to pulmonary embolism (PE). Instead, the best data we have are cohorts of patients with AF but no prior venous thromboembolism (VTE). The question is whether they are at increased risk of subsequent PE. There are a number of studies that offer a sense of the strength of association. Here are three:
- The first is a study from 2015 that looked at 11,458 patients with newly diagnosed AF and no evidence of VTE. Subsequent VTE events were reported and compared with a group of patients who did not have AF. The incidence of VTE was higher in the AF group, even after adjusting for comorbidities, sex, and age, with a hazard ratio of 2.2.
- A second study, also from 2015, examined a cohort of 1,604 patients with AF. The rates of subsequent VTE were again assessed. AF increased the risk of PE with a hazard ratio of 11.8 and DVT with a hazard ratio of 6.2. The risk of VTE was particularly increased in the first 6 months after AF was diagnosed.
- Finally, a 2021 study of 463,244 AF patients without previous VTE, ischaemic stroke, or pulmonary hypertension were compared to 887,336 population controls. VTE rates were higher among AF patients during the first 30 days after an AF diagnosis with a hazard ratio of 6.6 in men and 7.6 in women.
There are a number of other studies showing similar associations. But, it is important to note that although most published literature supports a connection, some studies don’t show a link.
We can also look at autopsy studies. For example, in 1969 Hans Aberg reported that right atrial thrombus was present in 8.7% of patients with AF compared with 1.1% in those without AF.
Another autopsy study, this one from 1951, examined 51 cases of mitral stenosis and atrial thrombus. Twenty-four of 51 (47%) had a clot in the right atrium. In 27 cases, pulmonary emboli or infarcts were found. Sixteren had right atrial thrombus, and in 8 cases no other source of PE could be identified.
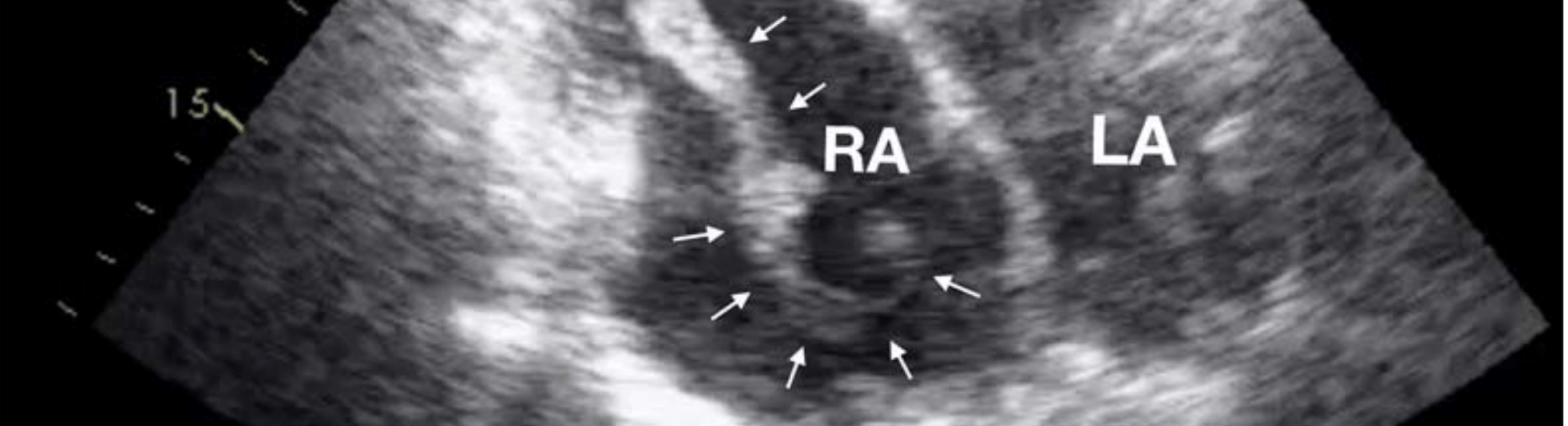
More contemporary echo studies similarly show that the RA is a site of thrombus formation.
The observation that not all patients with PE have DVT is also seen as support for the hypothesis that AF may cause PE. In fact, DVT is only found in about 50% of patients with PE. This is often taken as meaning the thrombus has already migrated. It could also mean there is a non-DVT source for the PE. Like the right atrium.
Looking at some of these studies reveals an unexpected association: AF is also associated with DVT. Understanding why AF might predispose to DVT requires a more complete review of thrombus formation. While it is certainly true that the chaotic atrial contractions lead to the stasis of blood, there is more to it.
Remarkably, AF affects all 3 arms of Virchow’s triad. Not only does AF lead to stasis, it is also a condition associated with endothelial injury and is considered a hypercoagulable state.
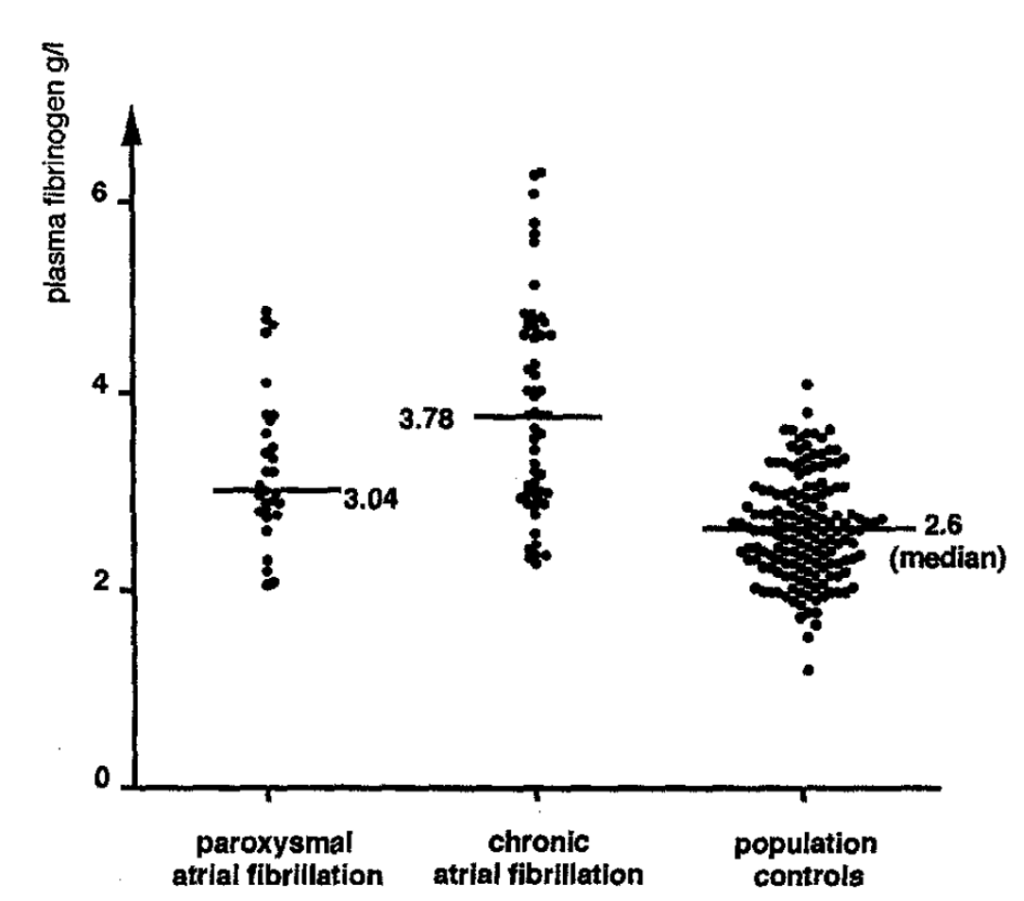
The hypercoagulability of AF could result from activation of the coagulation cascade, increased platelet reactivity, or impaired fibrinolysis. Turns out that each of these factors has been implicated in AF.
One example is the consistent finding of elevated levels of fibrinogen and d-dimer in those with AF. This has been seen repeatedly. In fact, the spontaneous echo contrast we see on imaging is partly due to RBC aggregation. And, of course, fibrinogen promotes the aggregation of RBCs. Similarly, markers of endothelial injury, including vWF, are elevated in patients with AF.
The exact mechanisms leading to the hypercoaguable state and endothelial injury are multiple and still being worked out. But they are there.
If one accepts that right atrial thrombus forms in AF and that these thrombi might embolize, one might wonder why we don’t see MORE pulmonary embolism with this condition. One reason is that most patients with AF are on anticoagulation. This may explain why the risk of PE is highest soon after AF is diagnosed. Patients may not be on anticoagulants yet.
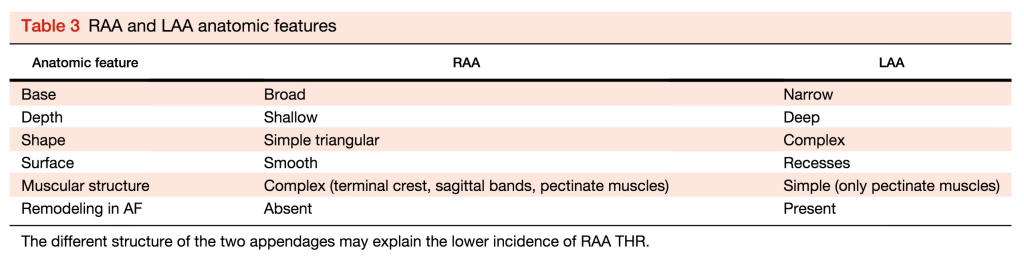
But, even accounting for this, PE is far less common than systemic embolization. Most commonly, stroke. One reason stems from the appearance of the right atrial appendage. Not only does the right atrium have an appendage, just as with the LA appendage, it is the most common site of thrombus formation. But it is also quite different in appearance compared to the left atrial appendage. It is broader and more shallow and lacks recesses. This, along with some other differences, likely contribute to the lower rates of RA thrombus.
Blood vessel size also plays a role. The main pulmonary arteries are pretty big compared to the cerebral arteries. Most atrial thrombi are between 2 and 20mm, though right atrial thrombi have been reported as big as 35mm. The main pulmonary artery is about 25mm with subsegmental pulmonary arteries measuring about 6-7mm.
The middle cerebral artery, in contrast, is between 3-3.5mm. Comparing the size of these arteries, it would make sense that cerebral emboli would be more likely to lead to obstruction and symptoms, at least compared with larger pulmonary arteries.
As one final note, the connection between AF and PE is supported by the fact that the CHA2DS2-VASc score predicts future PE in patients with AF.
Take Home Points
- Multiple studies demonstrate an association between atrial fibrillation and pulmonary embolism. The direction of causality is probably bilateral.
- Atrial fibrillation is associated with all three arms of Virchow’s triad: stasis, endothelial injury, and hypercoaguability.
- Pulmonary embolism is less likely than systemic embolism in those with AF. This is likely related to the anatomy of the right atrial appendage and to the diameter of the downstream vessels involved.
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (0.5 hours), Non-Physician Attendance (0.5 hours), or ABIM MOC Part 2 (0.5 hours).
Listen to the episode
https://directory.libsyn.com/episode/index/id/26451525
Link to associated tweetorial
Credits & Citation
◾️Episode written by Avi Cooper
◾️Show notes written by Avi Cooper and Tony Breu
◾️Audio edited by Clair Morgan of nodderly.com
Breu AC, Cooper AZ, Abrams HR. A Fib about PE. The Curious Clinicians Podcast. April 5, 2023.
This episode was sponsored by Green Chef!
Image credit: Cresti A, García-Fernández MA, Miracapillo G, et al. Frequency and Significance of Right Atrial Appendage Thrombi in Patients with Persistent Atrial Fibrillation or Atrial Flutter. Journal of the American Society of Echocardiography. 2014;27(11):1200-1207.
