
Why do we use a vaccine (BCG) to treat an unrelated malignancy (bladder cancer)?
This episode was dedicated to the intersection of infectious diseases and cancer. More specifically the use of Bacillus Calmette-Guerin (BCG), an attenuated form of Mycobacterium bovis, to treat a totally unrelated malignancy, bladder cancer.
First, some background. M. bovis is one of the many types of mycobacterium that can cause tuberculosis. And tuberculosis is defined as a disorder caused by mycobacteria in the M. tuberculosis complex, which includes M. tuberculosis, Mycobacterium bovis, Mycobacterium africanum, Mycobacterium microti, Mycobacterium canettii, Mycobacterium caprae, and Mycobacterium pinnipedii). BCG is most commonly used to treat bladder cancer via intravesical therapy.
Meta-analyses have shown reductions in tumor recurrence when BCG has been compared to control and other therapies including mitomycin C. To make the point that it is a live bacteria, there are many cases of disseminated BCG (i.e., disseminated M. bovis) after its use as a bladder cancer therapy.
To understand how to got to use BCG to treat bladder cancer we must go back to 1813. That year Arsène-Hippolyte Vautier reported that patients suffering from gas gangrene experienced a decrease in the size of their malignant tumors. An explanation wasn’t immediately apparent, partly because Vautier didn’t know the causative bacterium.
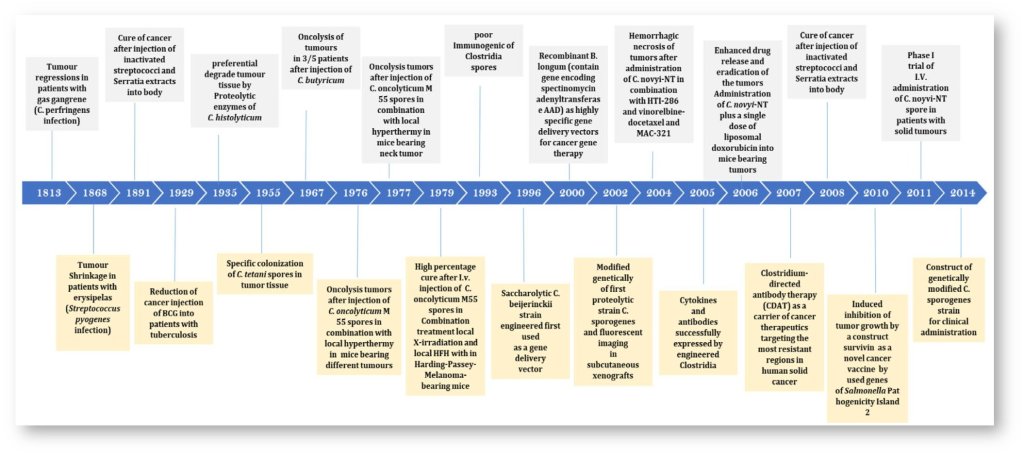
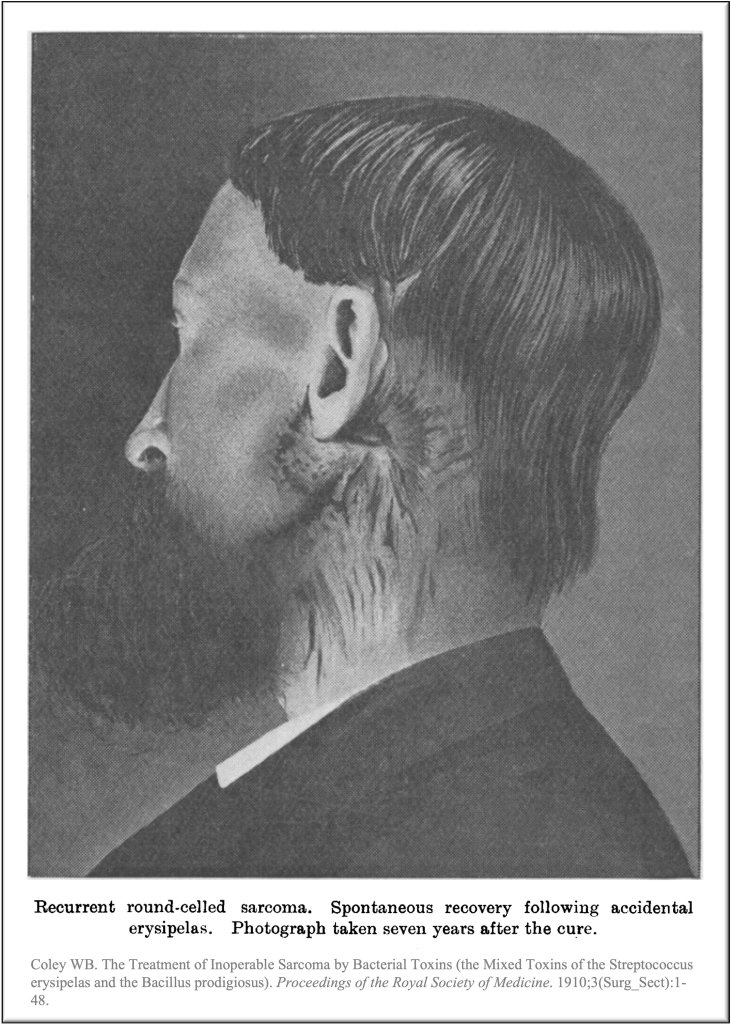
Decades later, Williams Coley heard about the curious case of a man with inoperable sarcoma that disappeared after erysipelas developed. The remission was durable out to at least 7 years. After hearing about this case, Coley wondered whether the intentional injection of Streptococcus pyogenes might work too. In 1893 he reported tumor regression in several patients with this therapy. He was so confident in these results that the first conclusion of this paper reads “the curative effect of erysipelas on malignant tumors is an established act.” The concoction came to be known as Coley’s toxins and it was used for decades.
Next, in 1929, Raymond Pearl reported another curious finding. In an autopsy study, he found a lower frequency of cancer in those with evidence of prior tuberculosis. Now it must be acknowledged that this study was later retracted after others noted that the study methods suffered from bias. Nevertheless, at the time the report spurred interest in whether other forms of mycobacterium might be used to treat cancer.
Based on Pearl’s findings and the reports of others researchers began to study BCG. First, BCG was tested in animal studies. Old et al found that BCG-infected mice showed increased resistance to tumors. In one experiment, the 48-day mortality was 0% in BCG infected versus 92% in uninfected controls.
The first trial of BCG in humans wasn’t actually for bladder cancer. Instead, it was for acute lymphoblastic leukemia. 30 patients with ALL in remission after chemo were treated. Relapse rates were 63% in BCG treated and 100% in controls
Many tumor types respond to BCG. Melanoma is another example. But bladder cancer emerged as the perfect option for this therapy because injecting the attenuated bacteria in the bladder allowed for a more controlled introduction to tumor cells.
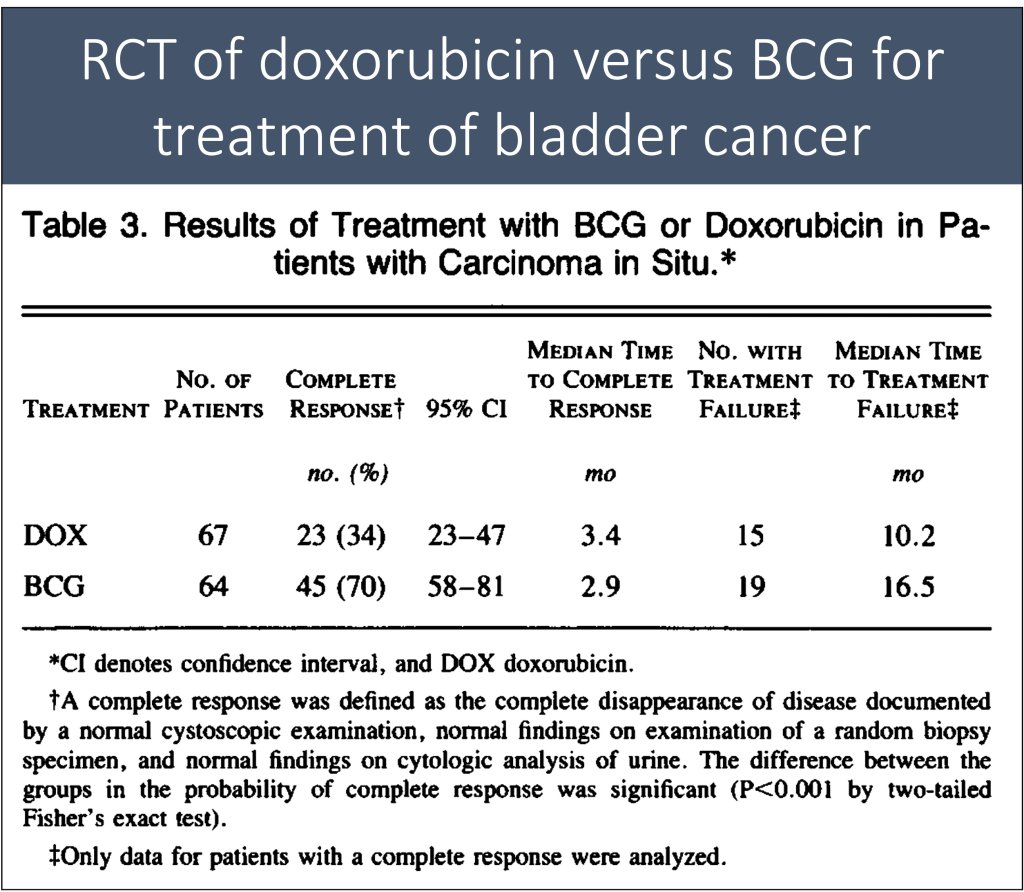
And the promise of BCG therapy in bladder cancer became clear with the results of a small trial published in 1976. The investigators treated 9 patients with recurrent non-muscle invasive bladder cancer with BCG and found a 12-fold reduction in recurrence. In subsequent years, BCG has also been compared head-to-head against chemotherapy – specifically doxorubicin – and proved superior. As noted earlier, meta-analyses have confirmed that it really does work.
How does BCG work? The easiest answer is that BCG is a form of immunotherapy. Studies have shown that BCG activates nearly all aspects of the immune system, including both innate and adaptive. And while we often equate the immune system with our fight against infectious diseases, it also has a key role in tumor recognition and rejection.
We see this play out in patients after solid order transplant. Their immunosuppression puts them at increased risk of cancers. On the other hand, the emergence of checkpoint inhibitors has really demonstrated well the power of immunotherapy.
We think of immunotherapy in terms of newer things like PD-1 inhibitors. But immunotherapy goes way back to Coley’s toxins. Whether it’s strep pyogenes or BCG, that the immune response to pathogens might “cross-react” with malignant cells is not surprising. And there are many other bacteria that have been used as immunotherapy including Salmonella, Clostridium, and many many others.
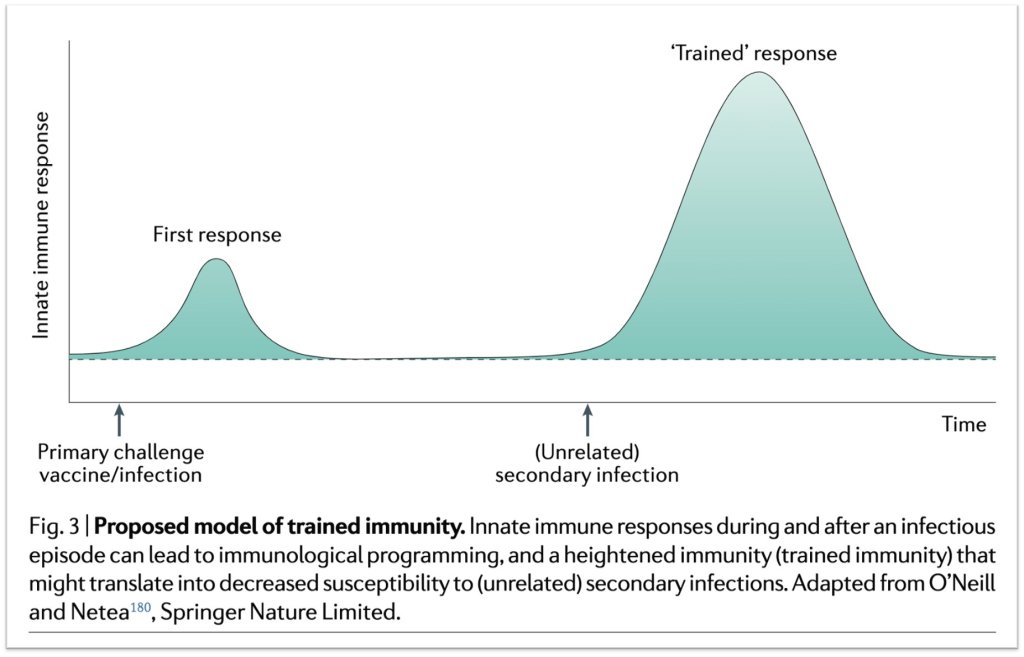
And BCG not only activates the immune system against cancer, it does the same other infections. One of the other mechanisms of benefit is something called Trained Immunity. This is the concept that innate immune cells (e.g., macrophages) “trained” by one infection or vaccine will respond with a heightened response to a second, unrelated, infection.
And there is data that BCG vaccination protects against not only TB but also unrelated infections like yellow fever, malaria, and even COVID. But please, just get a COVID vaccine. One recent RCT reported a decrease in new infections after BCG vaccination, particularly respiratory infections. I’ve really come to appreciate the power of BCG having read more about it.
Take Home Points
- For centuries bacterial have been observed to reduce tumor size
- These observations led to trials of BCG for cancer, including bladder cancer
- BCG acts as a form of immunotherapy, leading to immune destruction of cancer cells
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (1.00 hours), Non-Physician Attendance (1.00 hours), or ABIM MOC Part 2 (1.00 hours).
Listen to the episode
https://oembed.libsyn.com/embed?item_id=21690797
Credits & Citation
◾️Episode and show notes written by Tony Breu
◾️Audio edited by Clair Morgan of nodderly.com
Breu AC, Cooper AZ, Abrams HR. Infectious Cancer Therapy. The Curious Clinicians Podcast. January 5, 2022
Image credit: https://www.biorxiv.org/content/10.1101/2021.03.23.436651v1.full
Related tweetorial: https://x.com/tony_breu/status/1426587794202402816?s=20
