

Why does alcohol make one urinate so much?
For this episode, we discussed one of the most commonly used diuretics: alcohol. And we started with a very basic question. Can we explain the increased urination seen with alcohol consumption by simply looking at the fluid intake? If someone goes to a bar and has a few beers, of course they will urinate more.
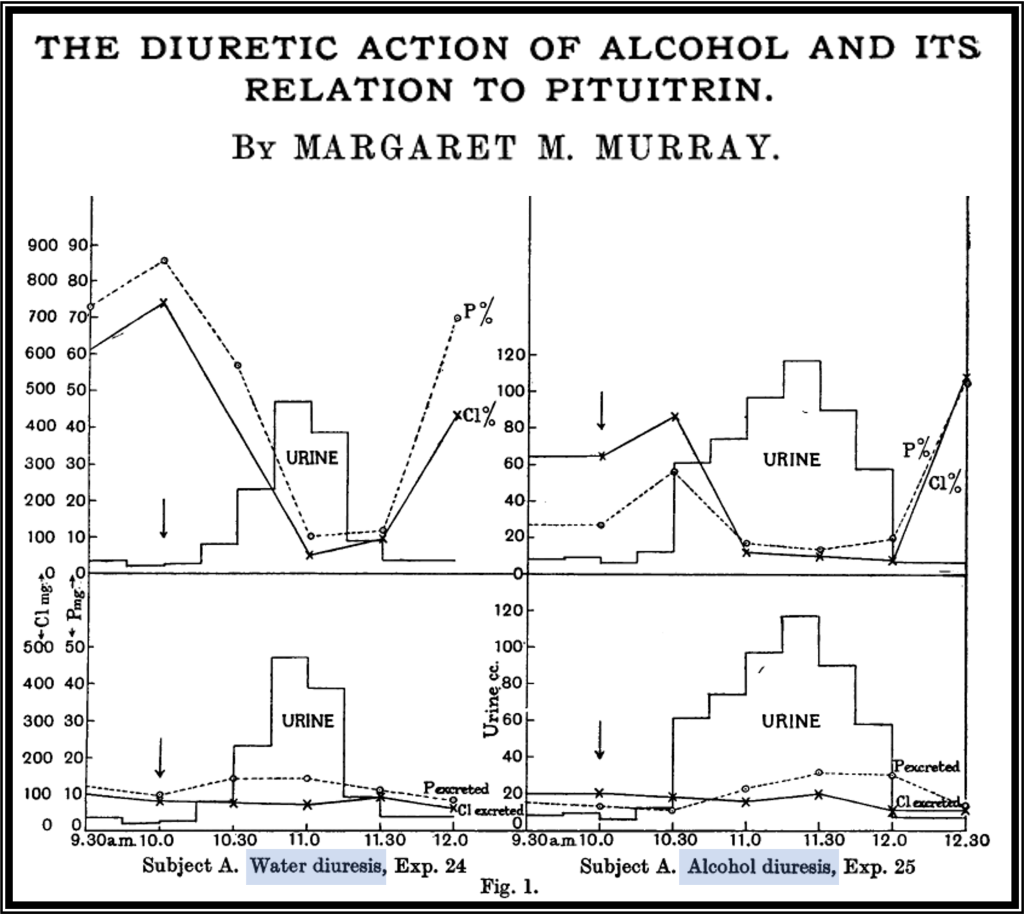
Fortunately, nearly 90 years ago studies were done to answer this first question. Margaret Murray published the key results in 1932. In the relevant experiments, Murray administered 300 mL or alcohol or water to two subjects and showed that alcohol led to more urine output than water alone. This suggested that there is something about alcohol – other than its volume – that causes a diuresis. But we didn’t yet know the mechanism.
To determine whether alcohol was leading to a solute diuresis or a water diuresis Kathleen Roberts performed a set of experiments with the results published in 1963. Roberts demonstrated that the urine osmolarity plummets from nearly 900 to less than 100 after ingestion of just 6-8 oz of 100 proof alcohol.
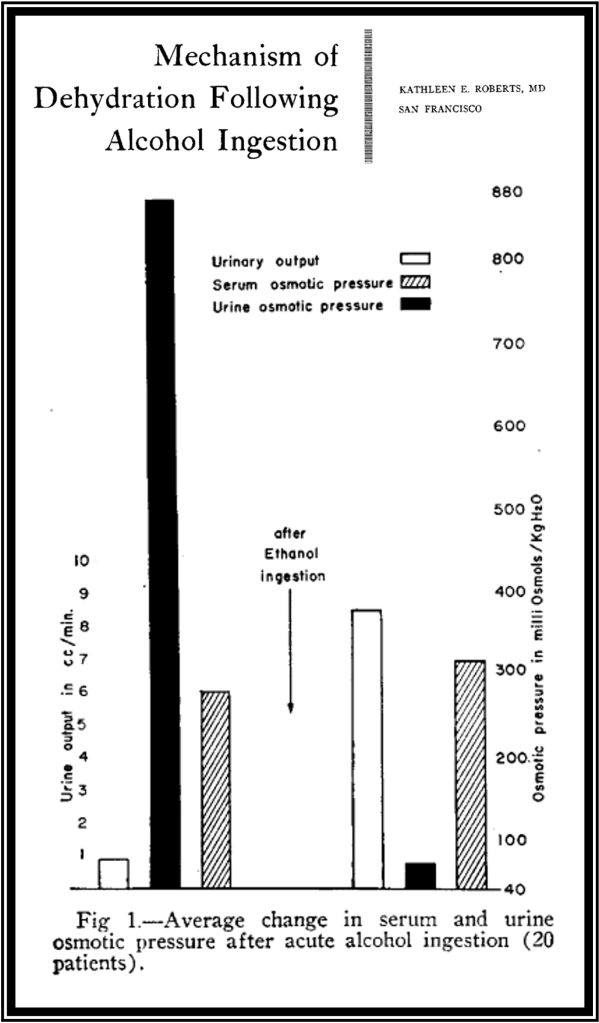
These results show that alcohol produces a water diuresis suggesting that it affects antidiuretic hormone (ADH). While you can get a water diuresis from the ingestion of large amounts of water the Roberts study showed a water diuresis occurred with small amounts of fluid ingestion. So it wasn’t from excess intake. Instead, ADH is affected. One way to think about it is that alcohol causes a form of diabetes insipidus (DI).
The final step was determining whether alcohol causes a form of central DI or nephrogenic DI. Going back to the study by Margaret Murry, there was a clue. In addition to just having her two subjects drink alcohol and water, she also performed additional experiments where she administered pituitrin alongside the alcohol or water. Pituitrin is an extract of bovine posterior pituitary hormones. It contains oxytocin and, more importantly, ADH. When Murray gave this with alcohol the diuretic effect was antagonized. This showed that alcohol has an effect on ADH release leading to a state similar to central DI.
Murray’s results were replicated and published in 1950. In that experiment, pituitary extract was administered. Doing so again blocked alcohol’s diuretic effect. This supported that the mechanism of action was a decrease in the release of ADH, as opposed to a decrease in its effect in the kidney.
In another experiment published in 1951 alcohol was injected directly into the carotid artery with the assumption being that it is delivered to the hypothalamus and/or pituitary. The result was a brisk diuresis.
And there have been more studies since showing that ADH levels rapidly decrease after ingestion of alcohol. The general consensus is that alcohol inhibits ADH release. And because ADH promotes water reabsorption, when it is lacking you there can be a profound water diuresis. Again, this of this as a form of very transient central DI.
Making use of this mechanism, alcohol has even been used as a treatment for the syndrome of inappropriate ADH (SIADH). In 1981, a patient with SIADH secondary to tuberculous meningitis was treated with alcohol. It worked, albeit transiently. And that’s because the effects are short-lived. So alcohol needs to be administered frequently, leading to intoxication and other problems. Clearly, we don’t use alcohol to treat SIADH but this is a cool demonstration of this physiologic mechanism.
There is even one report of alcohol being used to treat heart failure. This was in 1956, years before the release of thiazide and loop diuretics. It should come as little surprise that despite its ability to generate a water diuresis alcohol has not been used as a treatment for heart failure. It has been known to cause heart failure since the 1800s.
To combat the diuretic effect of alcohol one just need to turn on the mediators of ADH release: either increase osmolarity or become volume depleted. For example, in one study participants were given 200 mEq of sodium chloride on celery, just prior to their ingesting whiskey. This resulted in blunted alcohol diuresis. Similarly findings have been seen when you volume deplete patients before they drink alcohol.
As for the warning that once you “break the seal” you won’t be able to stop urinating, this pereception may relate to the delay in diuresis. The half-life of ADH is 15-20 minutes. So, the time to maximum diuresis might be expected to occur at 90-120 minutes, the time required for the metabolism of circulating ADH. Once the water diuresis has begun, it continues until the ADH levels rebound. You’ve got central DI!
Take Home Points
- Alcohol very quickly inhibits ADH release causing a form of transient central diabetes insipidus
- This results in a delayed, but brisk, water diuresis
- Things that elevated serum osmolarity and cause volume depletion can block this effect
CME/MOC
Click here to obtain AMA PRA Category 1 Credits™ (1.00 hours), Non-Physician Attendance (1.00 hours), or ABIM MOC Part 2 (1.00 hours).
Listen to the episode
https://oembed.libsyn.com/embed?item_id=21111668
Credits & Citation
◾️Episode and show notes written by Tony Breu
◾️Audio edited by Clair Morgan of nodderly.com
Breu AC, Abrams HR, Cooper AZ.. Breaking the Seal The Curious Clinicians Podcast. November 10, 2021
Image credit: https://www.winespectator.com/articles/does-it-matter-what-you-drink
Related tweetorial: https://x.com/tony_breu/status/1034891335411675137?s=20
