
My aim with this post is to review some of the historical literature related to the use of calcium salts (and other therapies) for severe hyperkalemia. This summary is not meant to be exhaustive. I did not, for example, perform a systematic review. But I do believe that the studies included below are among the most important. They are referenced repeatedly in reviews and guidelines.
Let’s start in 1883.
Many reviews note that Sidney Ringer’s 1883 paper is one the earliest (if not the earliest) to describe the benefits of calcium in hyperkalemia. Ringer’s paper is essentially a description of observations made as he exposed free hearts to all sorts of mixtures of electrolytes. Here is an example passage:
“If [calcium and potassium] are not present in the correct proportions then the trace becomes abnormal. If too little potassium is present, the contractions become broader &c. and there results fusion of the beats. If too much potassium is present, or too little lime salts, then the contraction of the ventricle is imperfect, and by increasing the quantity of potassium salt the beat becomes weaker and weaker till it stops.“
Ringer’s article has been offered as an early example of the dangers of hyperkalemia; I suspect this experiment is some of that evidence. And what about the antagonizing effects of calcium? This passage may be what others have taken as Ringer’s proof:
“After the ventricle supplied with saline and bicarbonate solution to which potassium chloride solution has been added, had stopped, I could always restore good contractions by the addition of from 3.5 c.c. to 5 c.c. of calcium chloride solution to the 100 c.c. of circulating fluid, and the contractions became as good as at the commencement of the experiment with blood mixture.
I must say that this isn’t the clear evidence I was expecting. But, it does suggest calcium’s role in mitigating the negative effects of hyperkalemia.
The next paper – published in 1918 by Samuel Amberg and Henry Helmholz – is rarely mentioned in contemporary reviews. As you can see from the title, this paper examines the effects of sodium salts (e.g., 5% sodium chloride [NaCl]) on the toxic effects potassium.1
In studies of guinea pigs, Amberg and Helmholz found that 5% NaCl protects against the otherwise fatal effect of potassium chloride. Interestingly, this protective effect was NOT seen with 0.55% NaCl.
While Amber and Helmholz’s findings are often left unmentioned, Winkler, Hoff, and Smith’s 1939 study is repeatedly offered as early proof of calcium’s efficacy. The investigators were clear that they intended to examine calcium:
“Mixtures of calcium and potassium salts were injected simultaneously, to determine whether the excess of calcium would affect either the critical fatal concentration of potassium or the characteristic disorganization of the ventricular complexes.“
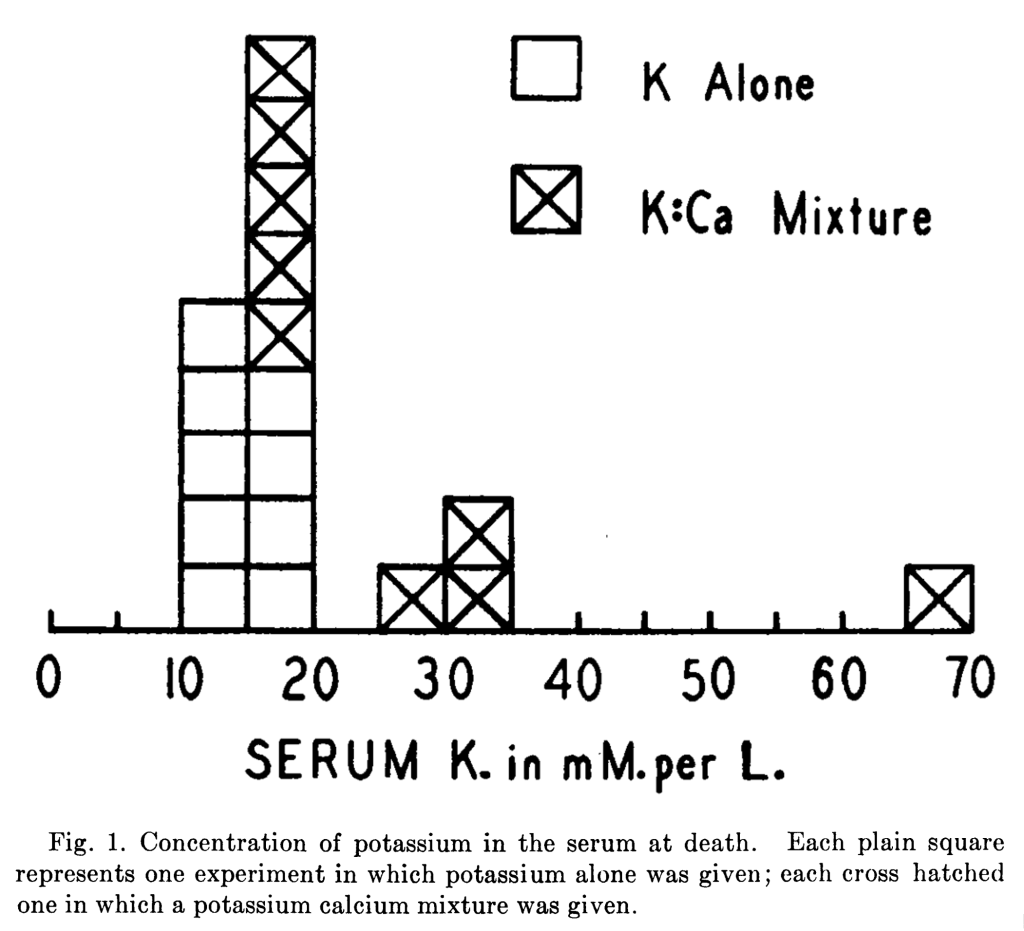
Dogs were injected with three types of solutions:
- 0.154 M potassium chloride (KCl) alone
- 0.154 M mixture of KC1 and calcium chloride (CaCl), the K:Ca molar ratio being 8:1
- 0.154 M mixture of KC1 and CaC1, the K:Ca molar ratio being 4:1
As Figure 1 shows, when KCl was given alone (i.e., without calcium), the serum potassium at which death occurs was lower than the values if calcium was added alongside the KCl. This was offered as evidence of the protective effects of calcium.
In 1946, Finch, Sawyer, and Flynn published a case report of two patients. Their observations are interesting. For example, they note that
“Calcium increased the frequency of ventricular contractions. The character of the complexes was not significantly changed and there was no resumption of auricular activity. It would appear, therefore, that calcium is useful only as a temporary measure to prevent cardiac standstill by increasing ventricular muscle irritability.”
It is unsurprising that calcium was found to be only temporarily effective. This has long been a presumed (and observed) characteristic of its use. That calcium “increased the frequency of ventricular contractions” suggests that the cardiac membrane becomes less stable (i.e., more excitable). This is the opposite of what I’ve been taught.
The authors also note that “Following administration of sodium chloride, both paralysis and electrocardiographic changes reverted toward normaI.” Their summary only mentions the use of sodium chloride, leaving out any discussion of calcium. I don’t want to read too much into this, but it suggests a stronger endorsement of sodium chloride than calcium salts.
John Merrill, Harold Levine, and Walter Somerville published another case report (10 patients), this one in 1950. The results with calcium were disappointing: “In our series, calcium in the amounts administered had little effect with the exception of Case 5, in which the change in serum calcium level may have played a role.”2
Just as with Finch, Sawyer, and Flynn, these authors found greater benefit with sodium chloride (in this case, 3% NaCl).
“Our experience indicates that the infusion of sodium may be of marked benefit where specific sodium depletion has played a role in the production of potassium intoxication. We have found that it is a more valuable agent than calcium but that its effect is temporary.”

Major W.H. Meroney and Lieutenant R.F. Herndon recorded data from the combat zone during the Korean War. In 1954, they published theirs observations on 46 patients who had sustained severe trauma, usually with massive blood loss and prolonged shock. They note that hypocalcemia is particularly important to monitor for in acute kidney injury because “calcium is a specific antagonist of potassium and hyperpotassemia and hypocalcemia occur at the same time.” In acute kidney injury, serum phosphate increases. This binds to calcium, resulting in a fall in calcium concentrations.

Meroney and Herndon noted that calcium “produces a striking improvement in the electrocardiogram“. This improvement is – of course – transient.
In what is becoming a theme of this early literature, sodium chloride was also beneficial: “Figure 5 shows the beneficial effect of raising the plasma calcium level followed by still further improvement from administration of sodium chloride.” This can be seen at the 30 minute mark.
The next study, published in 1955 by Silvio Weidmann, is key to our understanding of the mechanism of cardiac membrane stabilization with calcium. As I note in a Tweetorial on this topic, there are at least two ways that calcium might stabilize the cardiac membrane:
- Calcium might “undo” the increase in resting membrane potential (RMP) that hyperkalemia causes. This would mean returning the RMP to a more negative value (possibly back to -90 mV).
- Calcium might decrease the threshold potential. This would move it further away from the resting potential, making the cardiac membrane less excitable.
Weidmann showed that more depolarization was required in calcium-rich solutions. While the RMP was unchanged, the threshold potential had increased. Weidmann concluded that this increase in the threshold potential is what “accounts for the ‘stabilizing’ effect of Ca.”

Next, in 1956, Brian Hoffman and E.E. Suckling provide more evidence of the stabilizing effect of calcium. They write that “the effect of K on the resting transmembrane potential is dependent on the simultaneous Ca concentration. The interrelationship is such that the depolarizing effect of high K is decreased by elevated Ca and the depolarization produced by low K is diminished by low levels of Ca.”
They make no comment on the role of sodium chloride.
It should be noted here that hypertonic saline is not harmless. In 1959, Eliakim, Rosenberg, and Braun showed that rapid injection of 20% saline produced a number of potentially deadly ECG changes. But 20% saline is far more “hypertonic” than the 3-5% used in earlier studies.
In 1960, Sidney Greenstein and three co-investigators published their findings on the effect of sodium lactate, sodium bicarbonate, sodium chloride, glucose insulin, and calcium chloride for the treatment of induced hyperkalemia in nephrectomized dogs.
They found that “All these agents corrected the ECG evidences of hyperkalemia. However, sodium lactate appeared to be most efficacious in the correction of cardiac toxicity.”
Sodium chloride was inferior but provided some benefit. Calcium chloride was the least effective treatment tested.
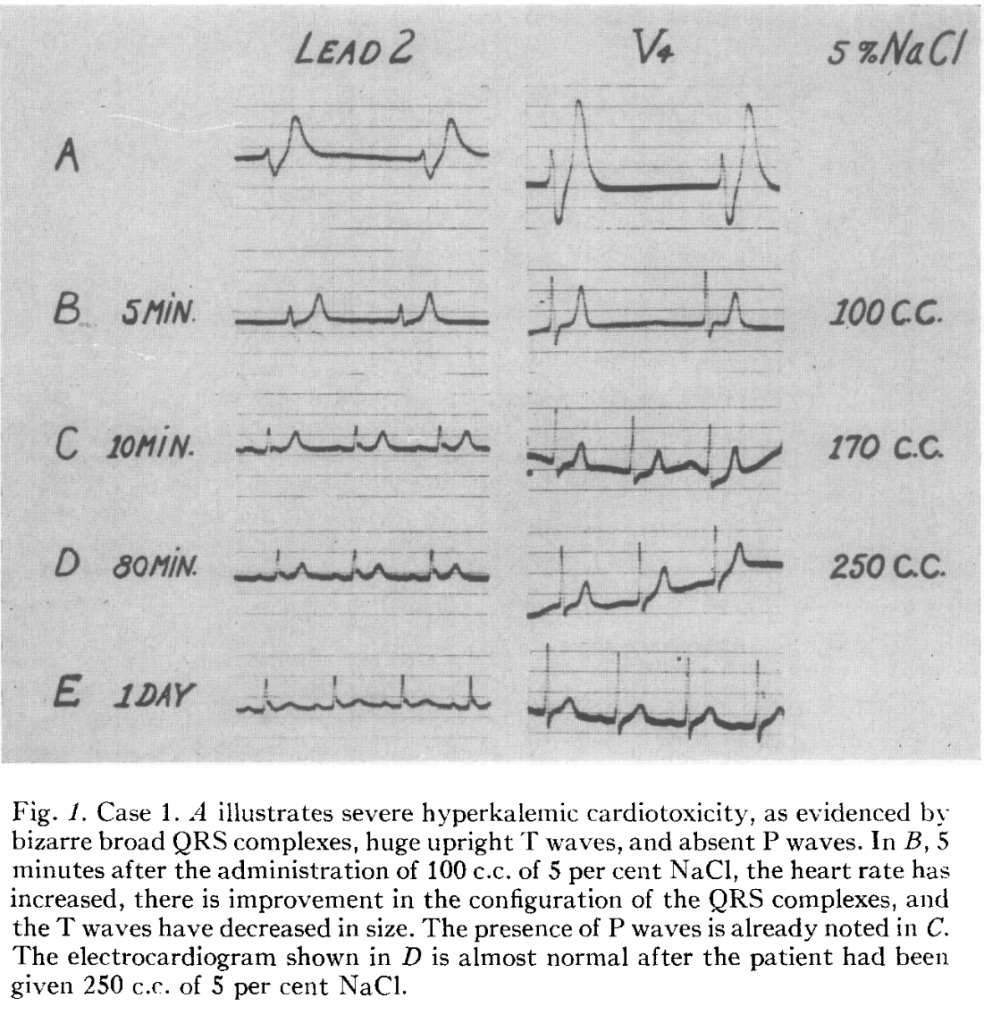
In 1962, Mario Garcia-Palmieri showed that 5% saline improved the ECG in 4 patients with hyperkalemia. Figure one is good case example:
At this point, here is where the tally stands:
- 1883 (Ringer; isolated ventricles): Calcium chloride may antagonize negative effects of hyperkalemia.
- 1918 (Amberg and Helmholz; guinea pigs): 5% sodium chloride protects against the otherwise fatal effect of potassium chloride.
- 1939 (Winkler, Hoff, and Smith); dogs: Calcium chloride effective protects against otherwise fatal effects of potassium chloride.
- 1946 (Finch, Sawyer, and Flynn; 2-patient case report). Calcium chloride, calcium gluconate, and sodium chloride improve ECG and symptoms.
- 1950 (Merrill, Levine, and Somerville; 10-patient case report): Calcium gluconate effective in 1 of 10 patients. 3% sodium chloride effective.
- 1954 (Meroney and Herndon; 46-patients): Both calcium salts and sodium chloride effective.
- 1955 (Weidmann; Purkinje fibers): Calcium stabilizes the cardiac membrane by increasing the threshold potential.
- 1959 (Eliakim, Rosenberg, and Braun; dogs): 20% saline is harmful.
- 1960 (Greenstein et al; dogs): Sodium lactate is best; sodium chloride is less effective; calcium chloride is least effective.
- 1962 (Garcia-Palmieri; 4-patient case report): 5% saline improved the ECG.
If I were a clinician practicing in the mid 1960s I don’t know that these set of data provides clear guidance on whether I should use calcium salts or hypertonic saline for severe hyperkalemia.
This brings us to a 1964 case report and review by M.J. Chamberlain and M.B. Birm. The authors review 5 cases where an immediate effect of calcium (either chloride or gluconate) on the ECG changes induced by severe hyperkalemia (serum potassium ranged from 8.6 to 10 mmol/L).
Though this report supports the use of calcium salts, it also notes that sodium chloride has been effective. “Of the other measures to combat hyperkalaemia, only rapid intravenous infusion of 5% saline solution (Garcia-Palmieri 1962) has such a rapid and dramatic effect.”
Their one-sentence conclusion reads as follows: “Intravenous injection of calcium is the treatment of choice in the emergency management of extreme hyperkalemia.“ While this case report supports the use of calcium, this conclusion seems rather narrow. This case report and review was published in The Lancet. I wonder if the clear conclusion and the weight of the journal began to change practice.
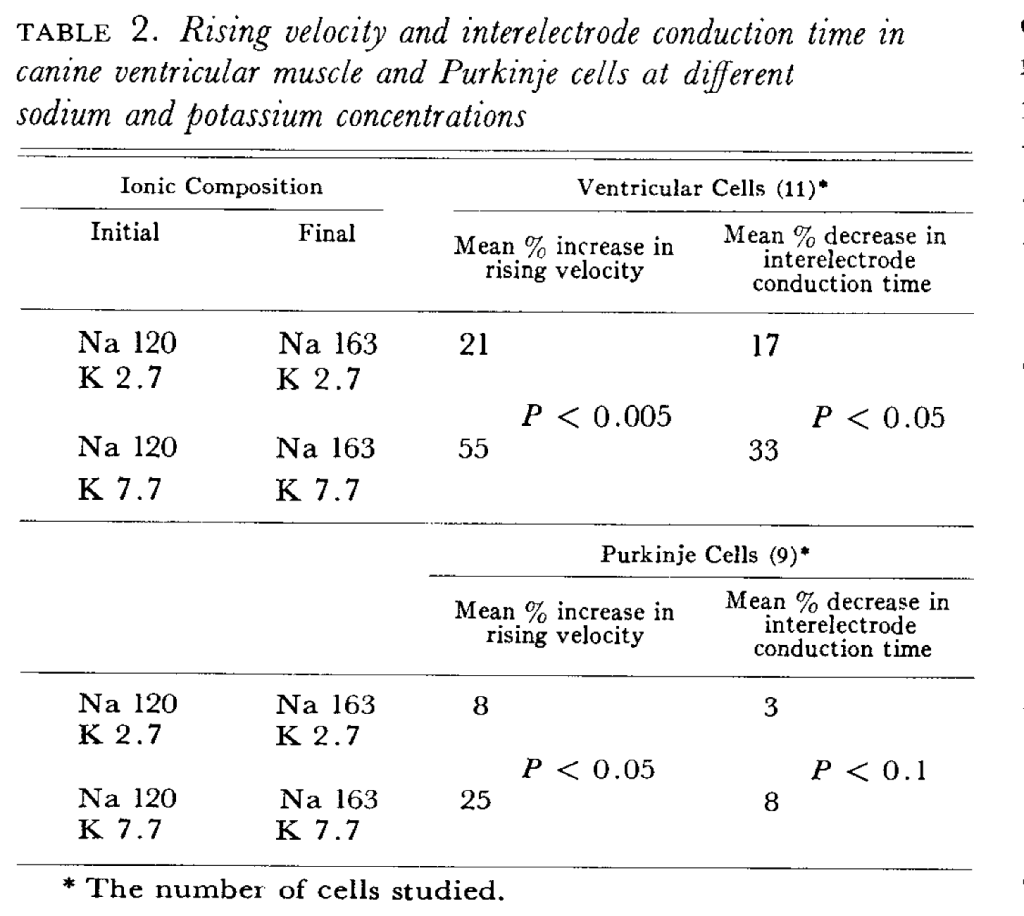
The final article in my review was published in 1975 by Ballantyne, David, and Reynolds. After nothing the prior literature suggesting a benefit of hypertonic saline, the authors show that a high sodium level mitigates the decrease in rising velocity that you get with hyperkalemia.
Table 2 shows the rising velocity (Phase 0) is significantly faster when the sodium concentration is increased.
There are undoubtedly other important articles in the “calcium to stabalize the cardiac membrane” arc. But I don’t believe I’ve left out any major ones. In reading these studies, I absolutely find support for the use of calcium salts (either calcium gluconate or calcium chloride). But I also find support for the use of hypertonic saline.
Older reviews mention both therapies, though calcium is clearly given greater weight.
For example, a 1966 a review of hyperkalemia published in The New England Journal of Medicine gave this recommendation for the treatment when there is severe cardiac toxicity: “calcium infusion is the most rapidly effective measure”. Later it mentions hypertonic saline by noting it will “counteract hyperkalemic toxicity, especially in hyponatremic or volume-depleted patients” But this review clearly sees calcium as the best therapy. It’s worth noting that this article provides no references.
Fast-forward to a 1975 review in JAMA that only mentioned calcium therapy. Notably, this was the same year that Ballantyne et all published their intriguing results on hypertonic saline. Reviews published over the last few decades all mention calcium salts as being the preferred therapy to “stabilize the cardiac membrane”. Some mention hypertonic saline, though rarely.
As the practice of medicine evolved, calcium salts won the day. This was clearly shown in a 1989 survey study published in The New England Journal of Medicine. Nephrology training-program directors were asked for their preferred therapy in severe hyperkalemia associated with renal insufficiency. IV calcium was the first choice therapy for 60% of respondents. There was no mention of hypertonic saline.
I doubt there will ever be a randomized clinical trial of calcium salts, either against placebo or head-to-head against hypertonic saline. I’m not sure it makes sense to ask for one. But, the story of how calcium salts emerged as the clear favorite fascinates me. It makes me wonder what other therapies have become the standard of care as potential alternates faded away.
I’d love to hear your thoughts. Comment below!
Notes
1Interestingly, the authors observe that it is actually urine that is toxic when injected. They surmise that it is the high concentration of potassium in the urine that is problematic.
2Remarkably, one review reported the exact opposite (i.e., they indicate that calcium was effective in 9 of 10 cases).

great insights
LikeLike
Beautifully researched and analysed
LikeLike
I am both grateful and amazed that people have the time and goodness to develop this kind of content. Thank you.
LikeLike
“Calcium might decrease the threshold potential. This would move it further away from the resting potential, making the cardiac membrane less excitable.”
I’m confused. I thought calcium increased the threshold potential. 🧐
LikeLike